
89.00$ Original price was: 89.00$.79.00$Current price is: 79.00$.
Sustaplex 275 10ml Top USA
Sustaplex 275 mg 10 mL XT Labs is a multi-ester testosterone blend designed to deliver both fast-acting and long-lasting anabolic effects. Each milliliter contains 275 mg of testosterone distributed across four esters: testosterone propionate (30 mg), testosterone phenylpropionate (75 mg), testosterone isocaproate (70 mg), and testosterone decanoate (100 mg). This combination was modeled after the original Sustanon 250 formula, but with a slightly higher concentration, offering athletes and patients a more potent option in the same 10 mL vial presentation. The inclusion of short, medium, and long esters ensures a quick rise in serum testosterone levels within hours of injection, while also providing a sustained release for up to two to three weeks. For bodybuilders, Sustaplex 275 is valued for its ability to drive significant gains in strength and muscle mass, particularly in bulking cycles, while in testosterone replacement therapy (TRT), it is used to restore normal physiological levels and alleviate symptoms of hypogonadism. Its balanced formulation makes it a versatile and powerful testosterone product, widely recognized in both clinical and performance-enhancement contexts.
Description
Sustaplex 275 XT Labs Composition Uses in TRT & Bodybuilding
Sustaplex 275 (Xt Labs) is an injectable testosterone blend containing four different esterified forms of testosterone. It is formulated similarly to the well-known Sustanon 250 blend, but with a total of 275 mg of testosterone per mL. This multi-ester composition was designed to provide both rapid onset and sustained release of testosterone in the body balance. In this deep dive, we will explore each ester in Sustaplex 275, the rationale behind such combinations, the historical development and use of Sustanon/Sustaplex for Testosterone Replacement Therapy (TRT), its prevalence in countries like the USA and Mexico, its role in bodybuilding for muscle mass gains, and how it compares to single-ester testosterone preparations (cypionate, enanthate, propionate). We will also discuss dosing strategies – from standard schedules to daily micro-dosing – and their effects on hormone stability and outcomes.
Composition of Sustaplex 275 XT Labs and Its Testosterone Esters
Sustaplex 275 is a Sustanon-style testosterone blend formulated at 275 mg/mL in a 10 mL vial. Its design combines short-, medium-, and long-acting esters to deliver both a rapid onset and a sustained release of testosterone.
Formula at a Glance (per 1 mL)
-
Testosterone Propionate — 30 mg
-
Testosterone Phenylpropionate — 75 mg
-
Testosterone Isocaproate — 70 mg
-
Testosterone Decanoate — 100 mg
Ester-by-Ester Breakdown
Testosterone Propionate (30 mg)
-
Half-life: ~2 days
-
Role in the blend: Provides an immediate rise in serum testosterone within hours of injection (“fast kick-in”).
-
Practical note: As a stand-alone ester it typically requires very frequent injections (daily or every other day) to maintain stability.
Testosterone Phenylpropionate (75 mg)
-
Half-life: ~4–5 days
-
Role in the blend: Extends the early phase of release; peaks a bit slower than propionate and helps sustain elevated levels through the first several days.
-
Practical note: Bridges the gap between very short and intermediate esters.
Testosterone Isocaproate (70 mg)
-
Half-life: ~9 days
-
Role in the blend: Provides a medium-term release profile (similar in feel to enanthate), maintaining testosterone as the shorter esters taper.
-
Practical note: Helps smooth the mid-cycle portion of the pharmacokinetic curve.
Testosterone Decanoate (100 mg)
-
Half-life: ~15 days
-
Role in the blend: Longest-acting component; delivers a slow, steady tail that can remain active for 2–3 weeks, supporting levels toward the end of the dosing interval.
-
Practical note: Reduces how often injections are needed if one accepts more fluctuation; with higher frequency schedules it helps flatten the curve further.
Why Use Four Esters?
Combining esters of different lengths is intended to layer release rates:
-
Immediate coverage: Propionate raises levels quickly in the first 24–48 hours.
-
Early sustain: Phenylpropionate maintains the initial elevation over the next few days.
-
Mid-range support: Isocaproate carries levels through the middle of the interval.
-
Long tail: Decanoate tapers slowly, extending overall duration.
This “cascading” profile aims to give a single injection both immediate effect and lasting coverage. All esters are ultimately hydrolyzed to the same active hormone (testosterone) once the ester chain is cleaved.
Important Note on “Ester Weight”
The labeled milligrams include the weight of the ester. Therefore, 275 mg of esterified testosterone ≠ 275 mg of free testosterone delivered. As a reference point, 250 mg of a Sustanon-type product yields ~176 mg of free testosterone after ester cleavage. Even so, the total steroid content and multi-ester design make Sustaplex 275 a robust androgenic-anabolic option, comparable in effect to other high-dose testosterone injections when dosed equivalently.
Origins of the Sustanon Blend and Its Rationale
Sustanon (and its underground counterpart Sustaplex) was conceived in the 1970s as a multi-ester testosterone solution. Its creation by Organon represented a pivotal shift in hormone replacement therapy (HRT), aiming to combine the fast-acting and long-acting properties of different esters into one injection.
Development by Organon
-
Timeline: Early 1970s, with the launch of Sustanon 250.
-
Purpose: To reduce the frequency of injections required for men with testosterone deficiency while still maintaining physiological levels.
-
Marketing: Positioned as a “long-acting testosterone shot” that could be given every few weeks, thus improving patient compliance and reducing discomfort.
This design was particularly relevant at a time when intramuscular testosterone was the cornerstone of treating male hypogonadism.
Why Four Esters Were Selected
Organon combined four esters to achieve a staggered release curve:
-
Short ester (Propionate): Provides a rapid spike within the first 24–48 hours.
-
Medium esters (Phenylpropionate & Isocaproate): Cover the middle portion, maintaining levels as propionate fades.
-
Long ester (Decanoate): Extends the effect for up to two to three weeks.
The intention was to minimize peaks and troughs seen with single esters:
-
Propionate alone: Requires daily injections to avoid crashes.
-
Enanthate or Cypionate alone: Creates a large initial peak followed by a slow decline, which can leave valleys if injections are too far apart.
By layering these esters, Sustanon was promoted as one of the most effective and stable TRT options of its era.
Is Sustanon Truly Better?
Pharmacologically, testosterone is testosterone. Once esters are cleaved, the hormone is identical regardless of form. Sustanon’s advantage was in its convenience and smoother release, not in producing different physiological effects.
However, clinical research revealed challenges:
-
A 250 mg injection every 3–4 weeks led to very high peaks (~70 nmol/L) in the first 48 hours, followed by declines back to baseline by week three.
-
Estradiol levels also spiked—up to double the normal range—triggering estrogenic side effects like breast tenderness.
-
Average testosterone over the cycle was mid-normal, but the fluctuation between peak and trough remained significant.
This showed that while decanoate does extend release, the shorter esters produce sharp early surges, meaning Sustanon can still cause instability if dosed too infrequently.
Modern Understanding and Clinical Implications
-
Groundbreaking in the 1970s: Sustanon’s multi-ester design was revolutionary as a “depot” testosterone injection that balanced immediate and sustained needs.
-
Current consensus: Injection frequency remains critical. To maintain stable levels, more frequent dosing (weekly or even every 5 days) is often required.
-
Practical outcome: Without optimized schedules, Sustanon can cause the same “peaks and valleys” it was designed to prevent.
Sustanon (Sustaplex XT Labs) in Testosterone Replacement Therapy (TRT)
Use in Medical TRT
Sustanon (the pharmaceutical version of this 4-ester mix, 250 mg/mL) has been widely prescribed for hypogonadal men. It restores normal hormone levels and alleviates symptoms such as low libido, fatigue, and muscle loss.
-
Typical administration: intramuscular injection every 3–4 weeks (e.g., 250 mg monthly).
-
Geographic use: Historically preferred in the UK’s NHS and common across Europe and Latin America for hypogonadism and gender-affirming therapy.
-
Value: Designed to reduce injection frequency compared with single-ester options.
Efficacy of Sustanon in TRT
Clinical studies confirm its effectiveness:
-
Improves sexual function, mood, muscle mass, and energy.
-
Benefits are due to restoring testosterone to physiological levels, not because Sustanon is inherently stronger.
-
Its uniqueness lies in dosing convenience rather than pharmacological superiority.
Injection Frequency Adjustments
Although marketed as a monthly injection, clinical practice shows this is often too infrequent.
-
Modern adjustments: every 2 weeks, every 10 days, or weekly injections at lower doses.
-
UK guidance: some specialists recommend injections every 5 days for greater stability.
-
Gender-affirming therapy: typically 100–125 mg weekly or every 10 days.
-
Key takeaway: smaller, more frequent doses help stabilize levels and reduce side effects.
Optimal TRT Dosage
-
General range: 100–150 mg per week (~0.4–0.6 mL of Sustaplex 275).
-
Traditional: 250 mg every 3–4 weeks – often causes a spike followed by a symptomatic crash.
-
Modern regimen: ~80 mg twice weekly, or ~125 mg every 7–10 days.
-
Clinical note: Regular monitoring and individualized adjustment are crucial.
Availability: USA vs. Mexico
-
USA: Sustanon/Sustaplex is not FDA-approved. Doctors prescribe cypionate or enanthate instead. Sustanon is only available through underground sources.
-
Mexico: Sold legally as Sostenon 250, manufactured by Aspen and other labs. Available in pharmacies as ampoules or pre-loaded syringes. Commonly prescribed for TRT under medical supervision.
-
Global difference: While the U.S. relies on single esters, Sustanon remains a standard TRT medication in many countries.
Carrier Oil and Tolerability
-
Formulation: uses arachis oil (peanut oil) with high benzyl alcohol content (~100 mg/mL).
-
Issues:
-
Peanut oil can cause severe allergic reactions in sensitive individuals.
-
High benzyl alcohol may increase post-injection pain (PIP) and irritation.
-
-
Comparison: single-ester products like cypionate (in cottonseed oil) are often smoother to inject.
-
Underground versions (e.g., Sustaplex 275): oil and solvent content may vary, so injection comfort differs between batches.
Use of Sustanon/Sustaplex XT Labs in Bodybuilding for Muscle Gain
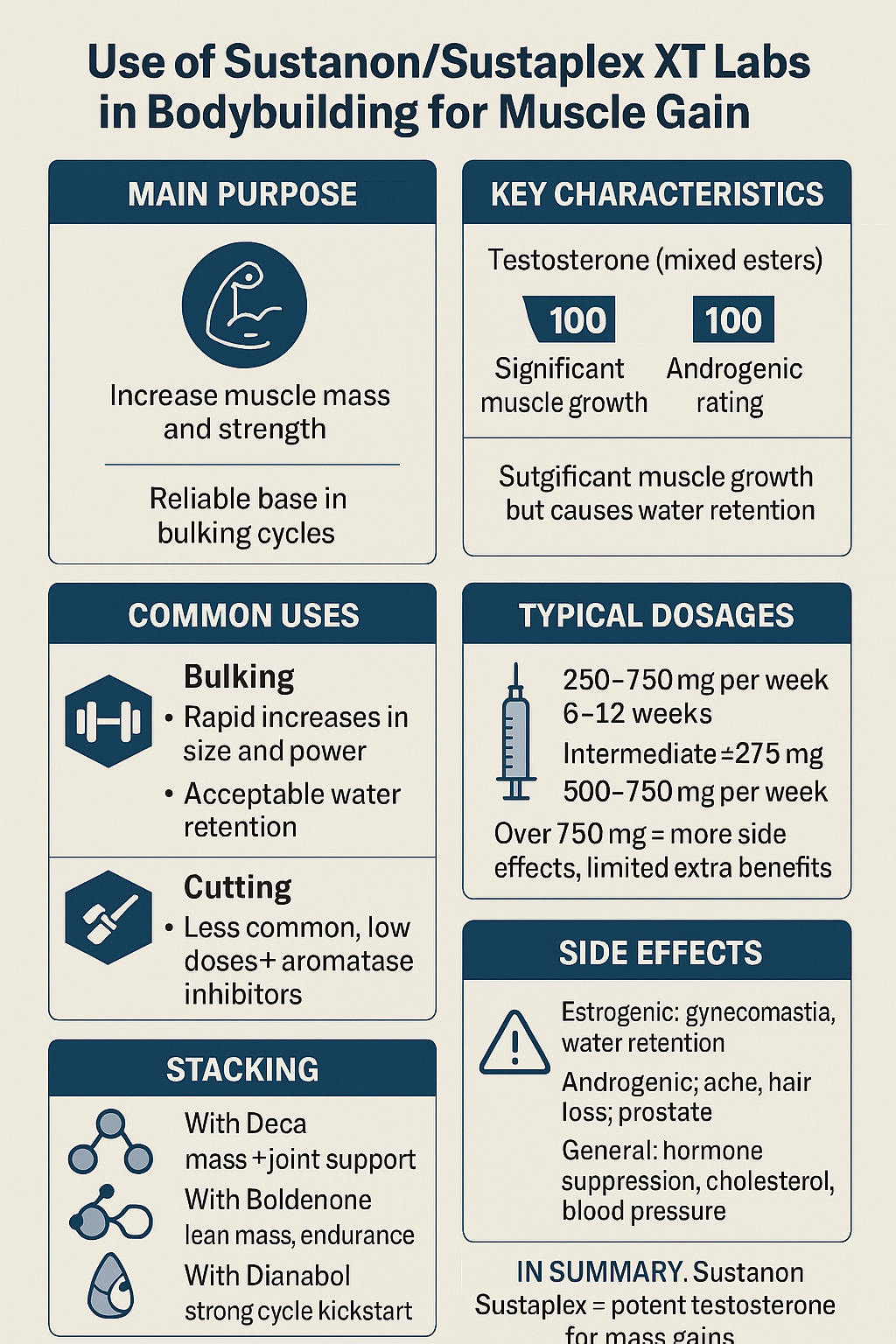
Aside from medical use, Sustaplex 275 (like Sustanon) is popular in the bodybuilding and athletic community as an anabolic steroid to enhance muscle mass and strength. Because it is essentially pure testosterone (just delivered in mixed ester form), it is a powerful anabolic agent with androgenic rating 100 and anabolic rating 100 (relative to testosterone’s baseline). Here’s how Sustanon/Sustaplex is viewed and used in the context of physique and performance enhancement:
Bulking cycles
Sustanon is most famously used as a bulking steroid for off-season muscle building. The robust androgenic-anabolic effects of testosterone lead to significant gains in muscle size and strength when combined with resistance training and adequate diet. Athletes often report rapid increases in weight and power. However, because testosterone readily converts to estrogen, Sustanon tends to cause moderate to high water retention in the body. The estrogenic activity (aromatization to estradiol) can lead to noticeable bloating, which actually contributes to strength (via improved leverage and hydration of muscle/connective tissue) but can blur muscle definition. For this reason, Sustanon is commonly reserved for bulking phases where maximum mass gain is the goal, and some extra water weight is acceptable. The water retention and estrogen also mean users must watch out for gynecomastia (male breast tissue growth) and manage estrogen levels if needed.
Typical dosages (bodybuilding)
Because Sustaplex 275 is a concentrated blend, bodybuilders typically dose it in terms of total mg of testosterone per week. Common cycle dosages are on the order of 250–750 mg per week, administered via injections once or twice per week. For example, an intermediate user might take 0.5 mL (≈137 mg) twice a week, totaling ~275 mg weekly, for a mild cycle; a more advanced bulker might inject 1 mL (275 mg) two to three times per week (550–825 mg/week). According to steroid guides, 250–750 mg every 7–10 days for 6–12 weeks can yield excellent gains. High doses beyond this (e.g. >750 mg/week) are generally considered to have diminishing returns – the muscle gains plateau, and side effects compound rapidly. In fact, reports suggest that even using Sustanon alone (without stacking other steroids) in the ~500 mg/week range “promotes good gains in mass and strength” for most users. Ultra-high “megadoses” (1 g+ per week) are sometimes attempted by hardcore users, but these greatly increase risks (severe HPTA suppression, blood pressure and cholesterol issues, etc.) and are not efficient since the androgen receptors can only be stimulated so much.
Stacking
In anabolic steroid cycles, Sustanon (testosterone) is often considered a base compound that can be stacked with other steroids. Common bulking stacks pair Sustanon with an anabolic that has lower androgenic effects, for synergistic growth. For example, a classic mass stack is Sustanon 250–500 mg/week plus Nandrolone Decanoate (Deca) ~300–400 mg/week – this combo was popular for its dramatic size gains (testosterone covers androgenic needs; nandrolone adds anabolic effect and joint support). Other combinations include Sustanon with Boldenone Undecylenate (Equipoise) for lean mass, or with an oral like Dianabol for a strong kickstart to the cycle. The Sustaplex blend’s advantage in a stack is simply providing testosterone (which is often deemed essential for maintaining normal physiological function and maximizing gains during any steroid cycle). In cutting (pre-contest) cycles, Sustanon is less commonly used because of the water retention, but if used, it might be at a lower dose (125–250 mg/week) alongside aromatase inhibitors to control estrogen, solely to preserve muscle while dieting.
Cycle length and PCT
Sustanon cycles usually run about 8–12 weeks. The presence of long decanoate ester means that after the last injection, testosterone release continues for several weeks. Bodybuilders plan their post-cycle therapy (PCT) timing accordingly – typically waiting around 3 weeks after the final Sustanon shot before starting PCT (with SERMs like tamoxifen or clomiphene) to allow hormone levels to drop. This is because if PCT is started too early while the long ester is still active, it won’t be effective. The decanoate in Sustanon causes a slow clearance; detection in blood can persist for over 3–4 weeks. This slow clearance is a double-edged sword: it helps maintain some anabolic effect between injections, but it also means a longer time to fully exit the system (relevant for both recovery and drug testing considerations).
In summary
In summary, Sustaplex/Sustanon is a powerful mass-building hormone. Bodybuilders value it for its efficacy in producing muscle gains, often stating that “testosterone is the base of any good cycle.” The multi-ester nature is not especially critical to muscle gains – it’s more about injection frequency convenience – but many athletes do appreciate that Sustanon kicks in fairly quickly (thanks to propionate) yet doesn’t need very frequent injections if they choose not to (thanks to decanoate). Most will still inject it at least weekly or twice weekly for more even results, as discussed below. The bottom line is that in the realm of performance enhancement, Sustanon’s reputation is that of a reliable, potent testosterone that can drive dramatic improvements in strength and size, albeit with the need to manage estrogen and other typical test side effects.
Comparing Sustaplex 275 (Sustanon Blends) to Single-Ester Testosterone (Cypionate, Enanthate, Propionate)

A long-standing discussion among both users and physicians revolves around whether a Sustanon-style blend is truly “better” or more stable than single-ester options such as testosterone cypionate, enanthate, or propionate. All of these deliver the same hormone—testosterone—but their pharmacokinetic profiles differ considerably, which impacts injection schedules, stability, and user experience.
Testosterone Propionate
Testosterone propionate is the shortest-acting ester, with a half-life of about 2 days. It peaks quickly in the bloodstream and also clears rapidly. This characteristic makes it especially useful for athletes looking for fine control of testosterone dosing, as levels can be adjusted within a matter of days. Because it clears faster than longer esters, propionate is often used toward the end of cycles or before competitions, since it can be discontinued a week before a drug test and will exit the system more quickly.
The main drawback is the frequency of injections required—daily or every other day—which makes it impractical for long-term TRT. Propionate also has a reputation for causing injection site pain, likely due to the solvent concentration. In blends like Sustanon, its role is to provide an immediate boost, but as a standalone option, it is rarely chosen for hormone replacement. For bodybuilding, however, it remains popular in short cycles or as a finisher to allow hormone levels to clear rapidly.
Testosterone Enanthate
Testosterone enanthate is one of the most widely used esters globally, with a half-life of around 5–7 days (some sources suggest up to 9). It is typically injected once a week, or split into two smaller doses weekly, making it a practical option for both TRT and bodybuilding.
Enanthate provides a relatively stable release curve: testosterone levels peak within a couple of days and then decline steadily over the course of 1–2 weeks. By day 14, levels are significantly lower but still present, making it possible to maintain therapeutic benefits for about two weeks. Clinical comparisons suggest that enanthate may provide slightly more stable levels than cypionate at the two-week mark, but in practice, the difference is negligible.
Enanthate is widely prescribed in Europe and is also available in the United States, though it is less common than cypionate. For TRT, enanthate performs reliably when injected weekly. For bodybuilding, it is a trusted compound that provides robust results, comparable to any other long-ester testosterone.
Testosterone Cypionate
Cypionate is extremely similar to enanthate and has a half-life of about 7–8 days. The chemical structure differs only by one carbon atom in the ester chain, making it slightly more oil-soluble and very marginally longer-acting. In practice, however, enanthate and cypionate are virtually interchangeable.
In the United States, cypionate is the dominant ester prescribed for TRT, usually at 100–200 mg per week. It is most often injected intramuscularly once a week, though some patients extend to biweekly injections. Many, however, report feeling best on weekly dosing to prevent end-of-cycle lows. A biweekly administration of 200 mg testosterone cypionate typically peaks within ~2–5 days, with estradiol rising in parallel. Mean serum levels then decline progressively, approaching baseline by the end of the two-week interval. This pharmacokinetic pattern illustrates why infrequent dosing leads to pronounced hormonal fluctuations(1)—a phenomenon equally observed with multi-ester testosterone blends.
One minor difference is the carrier oil: in the U.S., cypionate is frequently suspended in cottonseed oil, which is thinner and generally easier to inject. Enanthate, by contrast, often comes in sesame oil, which is thicker and sometimes causes post-injection lumps. Despite this, both esters are equally effective in terms of stability and results when dosed on a proper schedule.
Sustanon (Multi-Ester Blends like Sustaplex 275)
Sustanon represents a different philosophy: combining short-, medium-, and long-acting esters to cover both immediate and extended release. If used as originally designed—one injection every 3–4 weeks—it produces an early peak(1) (from propionate and phenylpropionate) followed by an extended tail (from decanoate).
However, this creates an issue. The early peak tends to be higher than with single esters at equivalent doses, but levels drop significantly toward the end of the interval. By the third week, testosterone is often at or near baseline, despite decanoate still releasing. This is why Sustanon, when injected only every 3–4 weeks, still causes peaks and troughs.
Modern practice has shifted toward more frequent injections, with many finding that every 5–7 days offers the best balance. Some TRT protocols even suggest every other day dosing, taking the propionate component as the limiting factor for true stability. With this approach, Sustanon can offer slightly flatter levels across a week compared to enanthate or cypionate, since the short esters cover the early phase while the long ester sustains the latter. Still, if one injects a single ester weekly, stability is equally good.
Which is Better?
The answer depends on context.
-
Sustanon/Sustaplex offers the advantage of some flexibility—if a dose is missed, the decanoate keeps a baseline level circulating. Some users also enjoy the quick “boost” from the propionate fraction in the first days after injection.
-
Single esters are simpler, easier to titrate, and more predictable. For doctors, cypionate and enanthate are preferred because their pharmacokinetics follow one clear decay curve, simplifying dose adjustments.
Region also matters. In the U.S., physicians almost exclusively prescribe cypionate or enanthate since Sustanon is not FDA-approved. In Europe and Mexico, however, Sustanon (marketed as Sostenon) is a standard medical option.
From a bodybuilding standpoint, the saying remains true: “testosterone is testosterone.” A 500 mg dose of Sustanon and a 500 mg dose of enanthate will produce essentially the same muscle gains and side effects if injected on equivalent schedules. Perceived differences like “Sustanon gave me less bloating” are typically anecdotal or due to injection timing, not inherent ester superiority.
Summary of Comparison
-
Propionate: short-acting, excellent control, impractical for TRT, ideal for short cycles.
-
Enanthate: long-acting, widely used, stable results with weekly injections, popular in Europe.
-
Cypionate: nearly identical to enanthate, dominant in the U.S., slightly different carrier oils.
-
Sustanon (Sustaplex 275): multi-ester blend with both fast onset and long tail, but not inherently more stable unless injected more frequently than originally designed.
In practice, all esters deliver the same hormone. The real difference comes down to injection frequency, availability, and personal preference.
Dosing Strategies and Stability of Sustaplex 275: From Weekly Injections to Daily Micro-Doses
When analyzing how to optimize the use of a multi-ester product like Sustaplex 275, one of the most important variables is injection frequency. Because Sustaplex 275 contains both short and long esters, the spacing of injections directly influences hormonal stability and the user’s experience. Over time, two main strategies have emerged: moderate doses at moderate frequencies (weekly or twice-weekly injections), and very frequent “micro” dosing, including daily injections of very small amounts. Both approaches aim to reduce the peaks and troughs in testosterone levels that often cause side effects.
Standard TRT and Bodybuilding Schedules with Sustaplex 275
In traditional TRT practice, Sustanon (and by extension Sustaplex 275) was prescribed as one full ampoule every 2–4 weeks. However, this approach is now considered suboptimal, as it creates wide hormonal fluctuations(2)‘. A more modern strategy involves injecting smaller amounts more frequently, such as every 7–14 days, to achieve greater stability.
In bodybuilding, the practice is even more precise. Athletes commonly split their weekly dosage into at least two injections per week (for example, Monday and Thursday). This method ensures that testosterone levels remain more even throughout the week. A typical example might be someone using 500 mg of Sustaplex 275 per week, dividing it into 250 mg on Monday and 250 mg on Thursday. This takes advantage of the overlapping esters and avoids the sharp surge that comes with a single large injection. Clinical observations also suggest that injecting every 5 days is a highly effective compromise, reducing the “peaks and valleys” while maintaining convenience. For instance, 300 mg of Sustaplex 275 every 5 days will maintain more consistent levels than 500 mg every 10 days, even though the total weekly amount is similar.
Daily or Very Frequent Micro-Dosing of Sustaplex 275
A more advanced approach is daily micro-dosing. Some TRT patients and bodybuilders inject small amounts every day to mimic the body’s natural rhythm of testosterone production. This strategy essentially eliminates hormonal peaks and troughs, resulting in extremely steady serum levels.
For example, instead of injecting 125 mg of Sustaplex 275 once per week, a user might inject about 18 mg per day (roughly 0.06 mL daily). This provides constant testosterone delivery and, according to anecdotal reports, can reduce side effect flare-ups such as mood swings, acne, or sudden spikes in estradiol.
However, when discussing 0.25–0.5 mL of Sustaplex 275 daily, the context shifts dramatically.
-
0.25 mL per day equates to ~68.8 mg daily, or about 481 mg per week.
-
0.5 mL per day equates to ~137.5 mg daily, or about 963 mg per week.
These amounts are far above TRT levels and firmly within bodybuilding “cycle” territory. At such dosages, the user maintains consistently high testosterone levels while benefiting from stable delivery. The advantage is smoother hormone profiles with fewer estrogen spikes, but the downside is that the overall exposure remains very high, leading to all the risks associated with supraphysiological testosterone use.
Benefits and Drawbacks of Daily High-Dose Micro-Dosing
The main advantage of daily injections at bodybuilding doses (500–1000 mg per week) is stability. Estrogen and DHT levels rise more gradually, which may help control side effects such as bloating or gynecomastia. Many users also report steadier energy, mood, and libido compared to the ups and downs of once-weekly injections. Additionally, smaller daily injections reduce post-injection pain and minimize scar tissue compared to larger, less frequent shots.
The disadvantages are clear as well. Daily injections require strict adherence, increase the risk of scar tissue buildup if sites are not rotated, and may be psychologically exhausting. More importantly, the side effects of high testosterone remain inevitable: polycythemia (elevated red blood cell count), hypertension, negative changes in cholesterol, testicular atrophy, oily skin, acne, and potential hair loss. At ~1 g per week (0.5 mL daily), the risk of requiring aromatase inhibitors to control estrogen is almost certain, and constant monitoring of blood pressure and cardiovascular health is essential.
Finding the Best Frequency for Sustaplex 275
For most users, the “best” injection frequency with Sustaplex 275 is a balance between stability and convenience.
-
Daily micro-dosing provides unmatched stability but is rarely necessary except for highly sensitive TRT patients or competitive bodybuilders seeking optimal hormonal smoothness.
-
Twice-weekly injections are the most common compromise, providing stable levels while avoiding daily hassle.
-
Every 5 days is another effective option, offering smoother profiles than weekly injections with fewer needles than daily protocols.
The key principle is to consider the shortest ester in Sustaplex 275 (testosterone propionate, half-life ~2 days) as the guiding factor. To avoid troughs, injections should ideally occur every 2–3 days. However, many users still feel well with twice-weekly schedules, while daily protocols remain a niche but effective method for those seeking absolute control.
Summary
Sustaplex 275 can be used in a variety of dosing strategies, from weekly injections to daily micro-doses, depending on the user’s goals. For TRT, smaller and more frequent injections (E3.5D, twice weekly, or even daily) help minimize side effects and maintain stable hormone levels. For bodybuilding, higher-dose micro-dosing provides a steady anabolic environment but does not eliminate the risks of running 500–1000 mg of testosterone per week. Ultimately, the best frequency is highly individual, with most users finding that twice-weekly injections of Sustaplex 275 strike the ideal balance between stability, convenience, and results.
Sustaplex 275 XT Labs Side Effects (Evidence from Sustanon®-Type Blends)
Sustaplex 275 (a Sustanon®-style, multi-ester testosterone blend) shares the risk profile of mixed-ester testosterone products. Below is an in-depth overview of Sustaplex 275 XT Labs side effects(3), synthesizing histopathology findings from experimental abuse of Sustanon® 250 (the reference pharmaceutical blend) and aligning them with known androgen/anabolic steroid (AAS) adverse effects. Note: the animal data summarized used very high, abusive doses (50–150 mg/kg/week for 12 weeks); risks at therapeutic TRT doses are lower, but the same organs and systems are potentially affected, especially with dose escalation, long duration, or pre-existing disease.
Key Takeaways at a Glance
-
Dose-dependence: Severity rises from 50 → 100 → 150 mg/kg (weekly IM), showing a clear dose–response pattern in liver, kidneys, and heart.
-
Organs most affected: Liver (hepatotoxicity), kidneys (nephrotoxicity), heart (cardiotoxicity).
-
Systemic AAS risks also noted: Atherosclerosis, tachycardia, cardiac hypertrophy, sudden cardiac death, mood/behavior changes (depression, aggression), GI upset, testicular atrophy, and general “liver injury.”
-
Translation to humans: Findings support caution with high-dose or prolonged Sustaplex 275 use and reinforce the need for monitoring even at TRT-aligned doses.
Hepatic (Liver) Side Effects of Sustaplex 275 (Sustanon®-Type)
Pathology observed with escalating abuse doses:
-
Hepatocyte degeneration and necrosis: Cell death increases with dose; patchy to more confluent injury.
-
Congestion and sinusoidal changes: Heavy congestion in the central vein and sinusoids; hemorrhagic areas can appear.
-
Inflammatory response: Macrophage infiltration, karyopyknosis, and focal hemorrhage indicate active injury and cleanup processes.
-
Architectural remodeling: Disrupted hepatic plates that rearrange into nodules, suggesting disorganized regeneration/fibrosis pathways under persistent toxic stress.
What this means for users of Sustaplex 275:
-
While TRT-range doses aim to minimize risk, high doses / long cycles can precipitate hepatocellular injury, congestion, and inflammatory changes. Clinically, this can translate to elevated AST/ALT, right-upper-quadrant discomfort, or, rarely, more serious cholestatic or hepatitic patterns—especially when combined with other hepatotoxic agents (e.g., oral 17-aa steroids, alcohol, acetaminophen).
Renal (Kidney) Side Effects of Sustaplex 275 (Sustanon®-Type)
Tubular and glomerular damage described:
-
Tubular epithelial degeneration and necrosis: Swelling, necrosis, and sloughing of the tubular lining cells; casts/hyaline material appear in lumens.
-
Bowman’s space alterations: Dilatation at lower doses; in other samples disappearance due to mesangial cell proliferation compressing the space.
-
Glomerular injury: Lysis/disappearance of some glomeruli at higher doses; congestion of glomerular capillaries.
-
Interstitial changes: Fibrosis and hemorrhage between tubules; precipitated inorganic material within tubules in some sections.
-
Epithelial proliferation/syncytia: Foci of tubular epithelial proliferation and syncytium formation indicate disordered repair.
Implications for Sustaplex 275 users:
-
Nephrotoxicity risk increases with dose and duration. Clinically, watch for rising creatinine/BUN, proteinuria, or hematuria. Dehydration, NSAID use, or concurrent nephrotoxins can amplify risk.
Cardiac (Heart) Side Effects of Sustaplex 275 (Sustanon®-Type)
Myocardial injury pattern with escalating exposure:
-
Myocyte degeneration and necrosis: Loss of cross-striations, cytoplasmic lysis, and pale/absent nuclei in affected fibers.
-
Hypertrophy and architectural derangement: Cardiomyocyte hypertrophy; at high doses, a “complete lack of normal architecture” with atrophied myofibrils.
-
Vascular changes and hemorrhage: Dilatation/congestion of intramyocardial vessels and hemorrhage between muscle bundles.
-
Syncytium formation: Disorganized myofibrillar syncytia appear with severe injury.
How this aligns with known AAS risks:
-
AAS abuse is linked to tachycardia, hypertension, atherosclerosis acceleration, arrhythmias, LV hypertrophy, heart failure, and sudden death. The histology above provides mechanistic backing for those clinical events—particularly under supraphysiologic dosing such as heavy cycles of Sustaplex 275.
Systemic & Endocrine Side Effects (Consistent with AAS Class Effects)
Beyond organ histology, the literature cited in the study (and broader AAS evidence) notes:
-
Cardiometabolic: Atherosclerosis progression, dyslipidemia (↓HDL, ↑LDL), hypertension, thrombotic risk.
-
Neuropsychiatric: Depression, aggressiveness/irritability, behavioral changes.
-
Reproductive/Endocrine: HPTA suppression, testicular atrophy, reduced sperm parameters, gynecomastia via aromatization to estradiol (especially at high doses).
-
Dermatologic: Acne, oily skin, androgenic alopecia in predisposed users.
-
Gastrointestinal: Nausea, vomiting, general “liver injury” symptoms when hepatotoxicity is present.
-
Hematologic: Polycythemia (↑hematocrit/hemoglobin), increasing viscosity and vascular risk.
Dose–Response, Duration, and Risk Modifiers
-
Higher weekly milligrams and longer exposure = more severe histopathology (liver/kidney/heart).
-
Stacking (multiple AAS, orals, stimulants) and poor injection practices raise complication rates.
-
Pre-existing disease (NAFLD, CKD, hypertension, dyslipidemia) magnifies risk even at lower doses.
-
Infrequent large injections may heighten peak-related adverse events (BP spikes, mood swings, aromatization), whereas more frequent split dosing can smooth kinetics but does not remove organ risks at supraphysiologic totals.
Red-Flag Symptoms & Monitoring for Sustaplex 275 Users (SEO-friendly Checklist)
-
Liver red flags: Dark urine, jaundice, RUQ pain, unexplained fatigue; labs: AST/ALT, bilirubin, ALP, GGT.
-
Kidney red flags: Foamy urine, flank pain, edema; labs/urine: Creatinine, eGFR, urinalysis (protein/hematuria), albumin/creatinine ratio.
-
Cardiac red flags: Chest pain, dyspnea, palpitations, reduced exercise tolerance, edema; tests: BP, lipids, ECG, echocardiogram when indicated.
-
Hematology: Hematocrit/hemoglobin (watch for polycythemia); consider phlebotomy guidance if elevated.
-
Endocrine: Total/free testosterone, estradiol (E2), LH/FSH (off-cycle), SHBG; prolactin if symptoms.
-
General: Periodic comprehensive metabolic panel (CMP) and lipid panel; consider cardiovascular risk scoring.
Practical Harm-Reduction Notes (TRT vs. Abuse)
-
Medical TRT targets physiologic levels with periodic labs and the lowest effective dose; this materially lowers risk.
-
Supraphysiologic “cycle” use of Sustaplex 275 (especially >500–1000 mg/week) places users squarely in the high-risk zone for hepatic, renal, and cardiac injury shown above.
-
If discontinuing after heavy use, anticipate HPTA suppression; medical teams often plan lab-guided recovery strategies.
Summary (Snippet-Ready)
Sustaplex 275 XT Labs side effects mirror those seen with Sustanon®-type blends: liver injury (necrosis, congestion, inflammatory infiltration, nodular remodeling), kidney damage (tubular necrosis/sloughing, Bowman’s space changes, glomerular lysis, fibrosis, hemorrhage, hyaline casts), and heart toxicity (myocyte degeneration/necrosis, hypertrophy, vascular congestion, hemorrhage, architectural loss). Systemic AAS risks—atherosclerosis, hypertension, dyslipidemia, mood changes, testicular atrophy, polycythemia—increase with dose and duration. TRT-level dosing with monitoring mitigates risk; abuse escalates it.
Sustaplex 275 Conclusion
Sustaplex 275 by XT Labs is a testosterone blend modeled on the classic Sustanon 250 formula, containing propionate, phenylpropionate, isocaproate, and decanoate esters of testosterone. Each ester plays a role in the timing of hormone release, giving the product both a fast onset and a prolonged action. This design was conceived to make testosterone replacement more convenient and to better mimic natural physiology, allowing for sustained testosterone levels with fewer injections.
Over the decades, Sustanon (and now Sustaplex) has proven to be an effective tool in both medical TRT and bodybuilding contexts. In TRT, it can restore virility, muscle strength, mood, and bone health in men with low testosterone, and it remains a staple in many countries’ hormone therapy regimens—particularly in the UK, Europe, and Mexico—while the U.S. largely relies on single esters. In bodybuilding, Sustanon’s high anabolic potency drives significant muscle and strength gains, making it a popular choice for bulking cycles despite its tendency to cause water retention.
When comparing Sustanon-type blends to single esters such as cypionate or enanthate, no form is inherently “better” in terms of anabolic results—all provide the same hormone and the same potential gains when dosed equivalently. The real differences are found in pharmacokinetics and convenience. Sustanon’s multi-ester formula was intended to provide more stable levels, but in practice it still requires relatively frequent injections to truly avoid fluctuations. Many physicians and users now administer Sustanon weekly or more often, achieving stability comparable to, or sometimes slightly better than, weekly enanthate injections, though in outcome the results are very similar. Single esters, meanwhile, offer simplicity and predictability, making them easier to fine-tune.
Dosing strategies have also evolved. Some individuals use frequent low-dose injections, even daily micro-dosing, to achieve nearly constant testosterone levels. This can reduce peaks and valleys, as well as side effects, in both TRT and bodybuilding cycles. However, for most users, a balanced approach such as twice-weekly injections suffices to maintain smooth, consistent levels.
The key takeaway is that Sustanon/Sustaplex 275 is a highly effective testosterone preparation, but the quality of results depends not only on its multi-ester composition but also on how it is used. Dose size and injection frequency matter just as much as the blend itself in determining whether the outcome is stable, effective, and well-tolerated.
Author
Evan D. Hart, PharmD, BCPS
Clinical Pharmacologist (Androgen Therapy & Performance Pharmacology) — Austin, Texas, USA
About
Evan D. Hart is a U.S.-licensed clinical pharmacologist with advanced training in androgen replacement therapy (TRT), ester pharmacokinetics, and performance-enhancing drug risk mitigation. He completed a Doctor of Pharmacy (PharmD), a PGY-1 pharmacy residency, and is a Board-Certified Pharmacotherapy Specialist (BCPS). Evan has led protocol design for outpatient testosterone therapy programs (IM, SC, and autoinjector modalities), and consults on dose-frequency optimization, hematologic safety (polycythemia), lipid management, and hepatic/renal monitoring for patients and clinics across the U.S.
Focus areas
-
Comparative pharmacokinetics of multi-ester blends (e.g., Sustanon-type) vs single esters (cypionate, enanthate, propionate)
-
Dose-splitting and micro-dosing strategies to reduce peak–trough variability
-
Adverse-effect surveillance: cardiometabolic, hepatic, renal, and endocrine risks
-
Risk communication for bodybuilding use vs. medical TRT; evidence translation into plain language
Public-facing work
Evan develops continuing-education content for clinicians, contributes to practical dosing frameworks used by U.S. TRT practices, and provides methodology reviews on PK modeling and safety monitoring checklists for androgen therapy programs.
Credentials (USA)
-
PharmD — United States
-
Board Certification: BCPS (Board of Pharmacy Specialties)
-
Practice location: Austin, Texas
-
Professional memberships: American College of Clinical Pharmacy (ACCP); Endocrine-focused pharmacy interest groups
Disclosures
Evan has no financial relationship with XT Labs or manufacturers of testosterone products. No paid endorsements. All writing is independent and evidence-referenced.
References:
1) Pastuszak AW, Gittelman M, Tursi JP, Jaffe JS, Schofield D, Miner MM. Pharmacokinetics of testosterone therapies in relation to diurnal variation of serum testosterone levels as men age. Andrology. 2022 Feb;10(2):209-222. doi: 10.1111/andr.13108. Epub 2021 Oct 8. PMID: 34510812; PMCID: PMC9293229. Pharmacokinetics of testosterone therapies in relation to diurnal variation of serum testosterone levels as men age – PMC
2) Shalender Bhasin, Juan P Brito, Glenn R Cunningham, Frances J Hayes, Howard N Hodis, Alvin M Matsumoto, Peter J Snyder, Ronald S Swerdloff, Frederick C Wu, Maria A Yialamas, Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 103, Issue 5, May 2018, Pages 1715–1744, https://doi.org/10.1210/jc.2018-00229
3) Al-Aubody, N. M., & Al-Diwan, M. A. (2018). Histopathological changes of liver, kidneys and heart of male rats caused by abusing of Sustanon® 250. Basrah J. Vet. Res, 17(3), 457-471. 457-HISTOPATHOLOGICAL-CHANGES-OF-LIVER-KIDNEYS-AND-HEART-OF-MALE-RATS-CAUSED-BY-ABUSING-OF-SUSTANON-R-250.pdf
Reviews
There are no reviews yet.