
Description
Decaplex 300 XT Labs (Nandrolone Decanoate 300 mg) – Uses, Benefits, and Side Effects
Decaplex 300 is a branded anabolic steroid solution by XT Labs, containing 300 mg/mL of Nandrolone Decanoate in a 10 mL vial. Nandrolone Decanoate – famously known by the pharmaceutical brand name Deca-Durabolin – is a synthetic derivative of testosterone classified as an anabolic-androgenic steroid (AAS). It was first introduced for medical use in the 1960s and became one of the most widely used AAS in both clinical therapy and bodybuilding contexts. Decaplex 300 provides a high-concentration formulation of this compound, typically intended for intramuscular injection. In this article, we delve into the scientific and medical research on Nandrolone Decanoate – the active chemical in Decaplex 300 – covering its therapeutic uses in medicine (anemia treatment, post-surgical recovery, burn injury, HIV-associated wasting, joint and bone conditions), its application in bodybuilding (muscle growth cycles and common steroid combinations), and an extensive review of its side effects and health risks.
What Is Nandrolone Decanoate (Decaplex 300)?
Decaplex 300 by XT Labs is a high-concentration injectable anabolic steroid formulation containing Nandrolone Decanoate (300 mg/mL), a long-acting ester derived from 19-nortestosterone—a modified testosterone molecule designed to maximize anabolic effects such as muscle and bone growth while minimizing androgenic side effects like hair loss or acne. Originally developed in pharmaceutical form as Deca-Durabolin, Nandrolone Decanoate was used medically to treat anemia and osteoporosis, thanks to its ability to promote red blood cell production, protein synthesis, and nitrogen retention. The decanoate ester gives the compound a prolonged half-life, requiring infrequent injections (every 1–4 weeks in therapeutic use) while maintaining stable anabolic activity. In the performance world, Decaplex 300 adapts this medical compound to the bodybuilding market, offering a higher concentration than traditional medical versions (50–100 mg/mL) to achieve effective muscle-building doses with smaller injection volumes. Athletes and bodybuilders use Decaplex 300 for its capacity to support significant lean muscle gains, enhanced recovery, joint relief, and increased strength, making it one of the most sought-after products in XT Labs’ lineup. However, despite its popularity, Decaplex 300 remains a potent hormonal compound whose non-medical use carries risks that require strict awareness and responsible management.
Medical Uses of Nandrolone Decanoate (Decaplex 300)
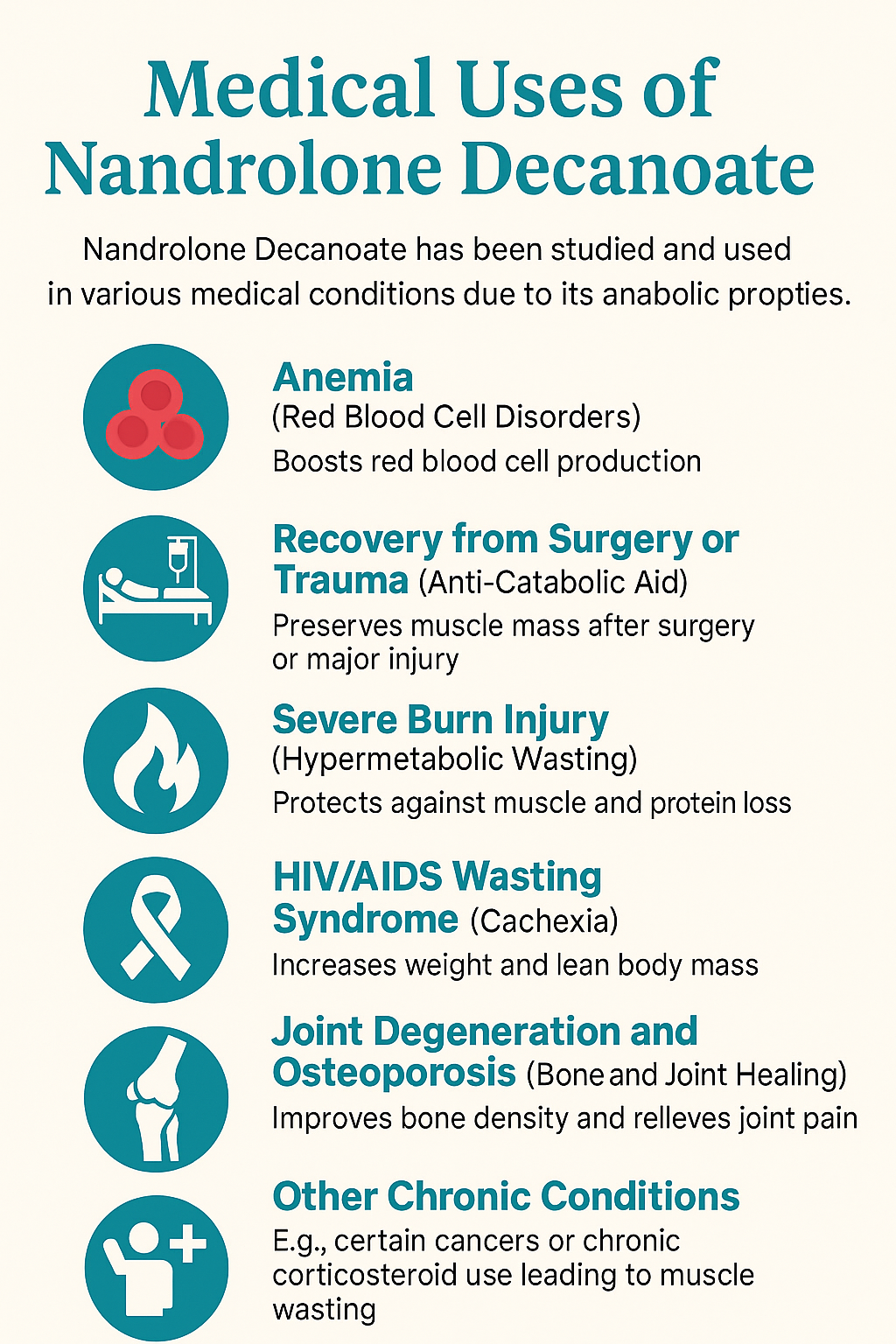
Nandrolone Decanoate has been studied and used in various medical conditions due to its anabolic properties (promoting tissue growth, red blood cell production, and nitrogen retention). The compound’s ability to stimulate erythropoiesis (red blood cell formation) and enhance protein synthesis made it a therapeutic option for certain debilitating illnesses. Its uses have evolved over time – some indications were common in past decades but have become less frequent as newer therapies emerged or due to concerns about side effects. The major medical (or investigational) uses of Nandrolone Decanoate include:
-
Anemia (Red Blood Cell Disorders)
-
Recovery from Surgery or Trauma (Anti-Catabolic Aid)
-
Severe Burn Injury (Hypermetabolic Wasting)
-
HIV/AIDS Wasting Syndrome (Cachexia)
-
Joint Degeneration and Osteoporosis (Bone and Joint Healing)
-
Other Chronic Conditions (e.g. certain cancers or chronic corticosteroid use leading to muscle wasting)
Each of these uses is discussed in detail below, citing recent scientific findings (especially post-2023 research where available) to assess Nandrolone’s efficacy and role.
Nandrolone Decanoate for Anemia Treatment
One of the primary historical medical uses of Nandrolone Decanoate is in the treatment of anemia, especially anemia associated with chronic illness. Anemia is a condition in which the body has insufficient healthy red blood cells to carry oxygen, leading to fatigue and weakness. Nandrolone can boost red blood cell production by stimulating erythropoietin (EPO) release from the kidneys and direct activation of EPO receptors in the bone marrow. It also appears to upregulate telomerase enzyme expression in hematopoietic (blood-forming) tissue, which may benefit certain bone marrow failure syndromes.
Clinically, nandrolone has been used to treat anemia of chronic kidney disease (CKD). Before synthetic erythropoietin (EPO) became widely available, anabolic steroids were a therapeutic option in CKD patients with anemia. Nandrolone was shown to increase hemoglobin levels in such patients by promoting RBC synthesis. According to the Cleveland Clinic, nandrolone is still sometimes prescribed for anemia in chronic kidney failure to improve red cell counts. For example, one study notes Nandrolone Decanoate is FDA-approved in the United States for anemia of renal disease (though currently no U.S. manufacturers market it)en.wikipedia.org. Typical medical dosages for anemia are relatively low (e.g. 50–100 mg intramuscularly every 1–4 weeks) – enough to stimulate erythropoiesis without excessive androgenic effects.
Beyond CKD, androgen therapy has shown benefits in aplastic anemia and other bone marrow failure conditions. Androgens like danazol, oxymetholone, and Nandrolone Decanoate have been used since the 1960s to stimulate blood cell production in acquired or inherited aplastic anemia. Recent research has revisited this approach for specific genetic bone marrow failures (e.g. Fanconi anemia or telomere-related disorders). A 2023 review in Haematologica noted that androgens can lead to hematologic responses in about 80% of patients with telomere diseases (like dyskeratosis congenita), often accompanied by telomere lengthening. In these studies, nandrolone decanoate was associated with fewer liver toxicity issues compared to oral androgens like oxymetholone or danazol, though it still caused virilization in a significant number of patients. Due to its intramuscular route, nandrolone avoids first-pass liver metabolism, potentially reducing hepatic strain for long-term therapy.
However, it’s important to emphasize that androgen therapy for anemia is now usually a last-resort or adjunct therapy. Modern first-line treatments (like immunosuppressants and bone marrow transplants for aplastic anemia, or EPO analogues for CKD anemia) are preferred due to better efficacy and safetyhaematologica.orghaematologica.org. Androgens are reserved for cases where standard therapies fail or are not available – for example, inherited aplastic anemia patients who cannot find a transplant donor may receive nandrolone to improve blood counts as a “bridge” to transplant. When used, nandrolone can partially alleviate transfusion dependence and improve blood counts in some patients.
From an evidence standpoint, current clinical trials are investigating nandrolone in these niches. An ongoing trial (NCT02055456) is evaluating Nandrolone Decanoate in telomere diseases (bone marrow failure with short telomeres) to see if it can safely improve blood counts. Early indications are positive on blood counts, but side effects like liver enzyme elevations and virilization are concerns. In summary, Nandrolone Decanoate is effective at stimulating red blood cell production, which underlies its benefit in anemia. This mechanism is the same reason bodybuilders often notice increased vascularity or endurance – higher RBC counts improve oxygen delivery. But in medicine, its use is cautiously weighed against side effects.
(Note: Athletes abusing Nandrolone may actually risk an excess of red blood cells (polycythemia), which can increase risk of blood clots. Regular blood tests are necessary in clinical use to ensure hemoglobin does not rise too high.)
Nandrolone Decanoate for Post-Surgical or Trauma Recovery
Severe trauma, major surgeries, or critical illnesses (like sepsis) often induce a hyper-catabolic state – the body rapidly breaks down muscle and lean tissue in response to stress and immobilization. Nandrolone’s potent anabolic effects made it a candidate to help patients recover lean mass and strength after surgeries or injuries. In the past, nandrolone decanoate was used pre- or postoperatively to counteract muscle wasting during prolonged recovery. For example, patients recovering from major surgery or long hospital stays were sometimes given anabolic steroids to prevent excessive weight loss and to speed rehabilitation.
Modern research continues to explore this. A double-blind controlled study in 2021 investigated small doses of nandrolone decanoate in patients after total knee arthroplasty (knee replacement). The goal was to see if anabolic steroids improve muscle strength and functional recovery post-surgery. The findings strongly suggested nandrolone improved postoperative outcomes, as measured by better knee function scores and increased muscle strength compared to placebo. Similarly, anabolic steroids have been examined in orthopedic surgery patients (like those after hip fracture repair) to reduce muscle loss and improve mobility during rehabilitation. These studies indicate nandrolone’s anti-catabolic effect can benefit recovery in musculoskeletal surgeries, especially in elderly patients at risk of sarcopenia (muscle loss).
Even outside orthopedics, nandrolone has been noted as useful in general trauma or critical illness convalescence. Historically it was given to patients with prolonged bed rest, major injuries, burns, or ulcers to promote tissue regeneration. By improving nitrogen balance and protein synthesis, nandrolone can help preserve muscle mass during immobilization. It also stimulates appetite in some cases, indirectly aiding recovery by improving nutritional intake. These benefits, however, must be balanced against risks like infection (anabolics can slightly reduce immune function or mask infections) and thrombosis risk if polycythemia develops.
Nandrolone Decanoate in Severe Burns
Severe burn injuries are one of the most hyper-catabolic conditions, as burn patients often lose large amounts of muscle and protein due to the body’s intense metabolic response needed for wound healing. Nandrolone Decanoate has been studied as a therapy in burn patients to improve outcomes. In 2022, Ali et al. published a randomized controlled trial in the journal Burns examining nandrolone in patients with 20–40% total body surface area burns. Forty burn patients were randomized to either standard care or standard care plus nandrolone decanoate injections during their recovery.
The results were very promising: the nandrolone-treated group showed preservation of lean body mass, improved protein balance, and near-normal nitrogen balance compared to controls. Clinically, this translated to better maintenance of muscle and possibly faster wound healing. The study concluded that nandrolone decanoate can be a safe and effective adjunct to combat the hyper-catabolic impact of burn injuries. Importantly, no serious adverse effects were noted during the treatment period in that trial, addressing concerns from older literature that anabolic steroids might complicate acute care. The authors suggested that after years of nandrolone being “recalled” (i.e., falling out of favor), it deserves re-evaluation as a burn therapy.
Nandrolone’s benefit in burns is akin to that of oxandrolone, another anabolic steroid which is actually FDA-approved for treating involuntary weight loss in severe burns. Oxandrolone has become a standard in many burn centers to help patients regain weight and strengthfrontiersin.org. Nandrolone, being injectable and longer-acting, could serve a similar role, especially in settings where daily oral administration is challenging. Its anti-catabolic effect preserves muscle mass, and it may also improve wound healing through increased protein synthesis and collagen deposition in tissues.
One consideration is that burn patients often have impaired liver and kidney function from the injury stress, and anabolic steroid dosing must be cautious. The 2022 study used a moderate dosing regimen (exact dose not stated in abstract, but likely around 25–50 mg weekly or biweekly for those patients). Significant improvements in weight and lab markers were observed, confirming earlier smaller studies and case reports that had suggested nandrolone could help in burn rehabilitation.
Nandrolone Decanoate and HIV/AIDS Wasting
During the height of the AIDS epidemic in the 1980s–1990s, patients with HIV frequently suffered from wasting syndrome – unintentional weight loss, muscle atrophy, and fatigue due to the infection and associated anorexia. Anabolic steroids were explored as a way to increase weight and lean body mass in HIV-positive individuals. Nandrolone Decanoate was one of the agents tested in clinical trials for HIV wasting, alongside others like testosterone and oxandrolone.
A seminal study by Gold et al. (published in AIDS 1996) investigated nandrolone in HIV-positive men who had lost 5–15% of body weight despite nutritional interventions. In this 16-week trial, patients received 100 mg of Nandrolone Decanoate intramuscularly every 2 weeks. The outcomes were impressive: patients experienced significant increases in body weight (about 0.14 kg per week) and on average gained ~3 kg of lean body mass over the 16 weeks. Body composition improvements were confirmed by multiple measurement methods. Perhaps just as importantly, quality-of-life scores improved significantly, especially in functional well-being. The study reported no significant toxicity; liver enzymes and other labs remained acceptable, and no virilization was relevant since the cohort was male. The authors concluded that nandrolone decanoate has beneficial effects on weight, lean mass, and quality of life in HIV-associated mild-to-moderate wasting.
Other studies around that time echoed these findings. For example, Dobs et al. 1999 found that nandrolone (at 600 mg doses monthly, or 150 mg biweekly) significantly increased lean mass in men with AIDS wasting compared to placeboswolverine.comswolverine.com. In HIV-infected women with wasting, a randomized placebo-controlled trial showed nandrolone therapy led to weight gain and lean mass accrual with a generally safe profilepubmed.ncbi.nlm.nih.gov. These studies collectively led to the acceptance of anabolic steroids as a treatment option for HIV wasting syndrome in the late 1990s. Indeed, nandrolone decanoate improved body weight, muscle mass, and overall well-being in patients with HIV according to multiple trials. One summary noted that selected patients with HIV wasting saw improved weight, lean body mass, and quality of life with nandrolone.
It’s worth noting that nowadays, with effective antiretroviral therapy, severe HIV wasting is less common. However, for patients who do experience cachexia (for example, due to late-stage disease or concurrent illnesses), nandrolone or other anabolic agents remain potential therapies. Nandrolone is often used off-label to preserve lean mass in HIV/AIDS patients. In practice, physicians might choose oxandrolone (an oral anabolic) for convenience, or megestrol acetate (an appetite stimulant) to promote weight gain. But nandrolone’s advantages include a strong anabolic effect and only biweekly injections.
One must monitor for side effects: in HIV-positive women, virilization is a concern; in men, testicular suppression and gynecomastia can occur. Still, the doses used medically (100–200 mg every 1–2 weeks) are modest compared to bodybuilding doses, and patients are monitored closely. A Cochrane review of anabolic steroids for HIV wasting (including nandrolone and testosterone) concluded that these agents significantly increase lean body mass and weight, though long-term effects on survival are unclear.
Joint Health, Bone Density, and Collagen Effects
An interesting facet of Nandrolone Decanoate (as found in products like Decaplex 300) is its reputed benefits on joint health and bone tissue. Anecdotally, bodybuilders have long claimed that “Deca” helps relieve joint pain – a claim that has some scientific backing. Nandrolone appears to increase collagen synthesis in connective tissues and improve bone mineralization, which can translate into stronger, more resilient joints and bones.
Joint Pain Relief
In 2020, Tatem et al. conducted a pilot study on men with hypogonadism (low testosterone) who had persistent joint pain. They added low-dose Nandrolone Decanoate to the patients’ hormone therapy. The results showed significant relief of joint pain in those men, with improved joint function and reduced discomfort, without major side effects noted in the short term.
This suggests nandrolone’s effects on connective tissue (possibly via collagen or water retention in joints) can ameliorate joint pain. Some hormone clinics now prescribe very low doses (e.g., 50–100 mg/week) of nandrolone alongside testosterone replacement in older men specifically for arthritic joint pain, and reports indicate noticeable improvements within weeks.
Mechanistically, nandrolone may boost synovial fluid production and collagen II content in cartilage, improving joint lubrication and cushioning. Its mild anti-inflammatory effect might also play a role in reducing joint discomfort. In practice, users of Decaplex 300 often reference these joint comfort effects during strength blocks.
Osteoporosis and Bone Density
Nandrolone was approved in various countries for treating osteoporosis in postmenopausal women. It exerts an anti-osteoporotic effect by inhibiting bone resorption and promoting bone formation. Clinical trials have demonstrated that nandrolone therapy increases bone mineral density (BMD) in women with established osteoporosis.
For instance, a double-blind 18-month trial in 46 postmenopausal osteoporotic women found that 50 mg nandrolone decanoate IM every 3 weeks significantly increased lumbar spine BMD by ~2.9%, whereas placebo patients lost BMD over the same period. Treated patients also reported less bone pain, and markers of bone turnover indicated a favorable shift (reduced collagen breakdown products, slight increase in bone formation markers).
Two patients did develop mild virilizing side effects (facial hair, voice deepening), highlighting the androgenic risk for women. Other studies (Hassager et al., 1990s) also confirmed nandrolone increases bone mass and reduces incidence of new fractures in elderly women.
Thus, nandrolone can improve bone density and strength, making it beneficial in osteoporosis and perhaps aiding fracture healing. In fact, some orthopedic research in animals suggests nandrolone enhances callus formation in fracture repair, which is often cited by athletes comparing medical literature to their experience with Decaplex 300 during recovery phases.
Mechanisms in Connective Tissue
Nandrolone’s ability to increase collagen has been documented. It preferentially stimulates Type III collagen synthesis, found in skin, ligaments, and tendon healing tissue. By promoting collagen deposition, nandrolone may strengthen tendons and ligaments, although there is a caveat: disproportionate collagen III can alter tendon properties, and there are reports of anabolic steroid abuse contributing to tendon rupture due to rapid muscle growth outpacing tendon adaptation.
Nonetheless, at therapeutic doses, nandrolone likely provides a net positive effect on connective tissues. Studies on rotator cuff injuries in animal models have shown nandrolone combined with exercise improved tendon healing and biomechanical strength of the tendon repair. These mechanistic insights are frequently discussed in guides that reference Decaplex 300 as a nandrolone decanoate option.
Clinical Joint Benefits
Beyond the research, decades of patient experience (especially in rheumatoid arthritis or degenerative joint disease) provide anecdotal evidence. Some older patients with arthritis who were given Nandrolone for osteoporosis noted less joint pain and improved mobility.
This has not become a mainstream indication, but it aligns with the notion that nandrolone’s anabolic effects on bone and cartilage can be symptom-relieving. The Cleveland Clinic health information also acknowledges that “some studies suggest nandrolone can help heal damaged joints.” For athletes, this is one reason Decaplex 300 is sometimes associated with “friendlier joints” during heavy training.
Other Medical and Investigational Uses
Aside from the major uses above, Nandrolone Decanoate has been tried or used in several other medical scenarios. References to products like Decaplex 300 in these contexts simply denote the nandrolone decanoate ester used clinically and anecdotally.
Chronic Kidney Failure (Non-anemic Effects)
In some countries, nandrolone was indicated for uremic patients (kidney failure) to improve nutritional status and hemoglobin. It can help CKD patients gain muscle mass and strength, which is beneficial as they often suffer muscle wasting (uremic sarcopenia).
It’s also been used to treat anemia in dialysis patients, as mentioned earlier.
Certain Cancers
High-dose anabolic steroids have an antineoplastic effect in specific cancers. Nandrolone was used in the past for inoperable breast cancer in women (before modern chemotherapy), aiming to slow tumor growth by the androgenic anti-estrogen effect.
Results were variable, and virilization side effects were significant, so this is now a rare usage. Androgens have largely been replaced by other hormonal therapies in breast cancer.
Long-term Corticosteroid Therapy
Patients on chronic glucocorticoids (e.g., for autoimmune diseases) often experience muscle and bone loss (steroid myopathy, osteoporosis). Nandrolone has been given in such cases to offset steroid-induced catabolism.
It helps maintain muscle and bone in patients who cannot discontinue corticosteroids, thereby reducing frailty. Some protocols that mention Decaplex 300 emphasize careful dosing and monitoring when catabolic steroids can’t be tapered.
Geriatric Frailty and Cachexia
In earlier decades, nandrolone and other AAS were tested in geriatric patients with general frailty, low weight, or “senile asthenia.” Some studies showed improved appetite, weight, and mobility in elderly men and women.
Today, this overlaps with treatment of conditions like COPD cachexia or cancer cachexia – any chronic wasting condition where anabolic support might improve quality of life. For instance, nandrolone has been studied as a pharmacological intervention for cancer cachexia, aiming to improve lean mass and physical function.
Pediatric Growth Failure
Decades ago, anabolic steroids were sometimes used in children with growth delay (e.g., constitutional growth delay or certain forms of dwarfism), to stimulate appetite and growth. Nandrolone was one such agent tried in selected cases of growth failure.
However, due to the risk of premature epiphyseal plate closure (androgen can cause bones to stop growing in length), this approach was largely abandoned in favor of growth hormone therapy for short stature conditions.
Nandrolone Decanoate in Bodybuilding (Decaplex 300 XT LABS in Physique Enhancement)
While Nandrolone Decanoate has legitimate medical uses, it is perhaps even more famous for its non-medical use in bodybuilding and athletics. In the sports world, Nandrolone (Deca-Durabolin) earned a reputation as a powerful bulking steroid that can add significant muscle mass and strength. According to the World Anti-Doping Agency, nandrolone is one of the most widely abused AAS in sports doping controls, and historically it has been “the most widely used AAS for physique and performance improvement” globallyen.wikipedia.org. Decaplex 300 by XT Labs is specifically marketed to this demographic as a performance-enhancing drug. Here we will discuss why and how bodybuilders use Decaplex 300 (nandrolone), including common cycles, stacking combinations, dosages, and the purported benefits that users seek. We will also address the legality and risks of such use.
Popularity and Appeal of “Deca” in Bodybuilding
High Anabolic Effect
Nandrolone Decanoate (Deca) has been a staple in bodybuilding since at least the 1970s. Its popularity stems from several factors:
As noted, nandrolone is highly anabolic, promoting substantial muscle protein synthesis and muscle hypertrophy. Users often experience significant gains in lean muscle mass when Deca is combined with proper diet and training. It’s a “mass-building” steroid, ideal for off-season bulking phases. Gains of several kilograms of muscle over a cycle are commonly reported.
Lower Androgenic Side Effects
Compared to testosterone, nandrolone causes relatively less androgenic issues like severe acne, hair loss, or aggressive behavior in many users. This is because nandrolone converts to a weaker androgen (dihydronandrolone) rather than potent dihydrotestosterone (DHT). For the bodybuilder, this means potentially fewer instances of hair thinning or prostate enlargement at equivalent muscle-building doses, and a generally “milder” feel on cycle (less risk of extreme aggression sometimes seen with high-testosterone or Trenbolone use).
Joint and Recovery Benefits
Athletes prize Deca for its joint-soothing effect. Many report that aches and pains from heavy lifting diminish on nandrolone. As discussed earlier, nandrolone increases collagen and water retention in connective tissues, lubricating joints and possibly improving recovery from injuries. In high-intensity training, this can allow the athlete to lift more comfortably and frequently. It’s often said that Deca helps “cushion” the joints – though this effect is partially due to water retention (which can also raise blood pressure).
Synergy with Other Steroids
Nandrolone stacks well with other compounds. It’s commonly used alongside testosterone and/or oral steroids to synergistically increase muscle gains. It’s not very liver-toxic (since it’s injectable), so it can be combined with other drugs without overwhelming hepatic stress. Also, nandrolone’s strong anabolic nature complements the androgenic effects of testosterone, yielding a more balanced cycle.
Long Half-Life and Stable Blood Levels
With the decanoate ester, Deca has a long half-life (~6–12 days). Bodybuilders find that a once- or twice-weekly injection schedule maintains stable blood levels. This is convenient and leads to steady gains without the frequent injections needed by shorter-acting steroids. The flipside is that it takes a while to kick in and also a long time to clear out (important for detection and recovery, discussed later).
Cultural and Historical Context (Pop Culture & Doping)
Classic bodybuilding literature often dubbed Deca as a relatively “safe” steroid (an oversimplification, as side effects can be serious, but relative to some others it was considered well-tolerated). It was famous enough to make its way into pop culture – for instance, Olympic sprinter Ben Johnson’s doping scandal in 1988 involved stanozolol, but many athletes in track and field later tested positive for nandrolone, illustrating its ubiquitous use.
Usage Patterns Across Populations
Surveys of AAS users frequently show nandrolone in the top five compounds used. It’s especially prevalent in off-season bodybuilders, powerlifters for strength, and even some recreational lifters. Female bodybuilders have sometimes used Deca in low doses, as it was thought to be milder androgenically (though virilization still occurs, so many women now avoid Deca in favor of milder anabolics).
Legal Status and Detection Risk
It must be emphasized: non-medical use of Nandrolone is illegal and banned in sports. Decaplex 300 is not a prescription pharmaceutical; it’s an underground lab product. Athletes in tested competitions risk multi-year suspensions if nandrolone metabolites are found in their urine. Nandrolone metabolites (19-norandrosterone) are notorious because they remain detectable for a very long time – sometimes up to 18 months after the last dose, due to the slow release from the decanoate ester and accumulation in fat tissue. This long detection window has caught many athletes off guard (some claimed their positive test was from “months ago” usage or even from contaminated supplements). For doping-tested athletes, nandrolone is one of the worst choices due to detection risk. For non-tested bodybuilders, that’s not a concern, but health is.
Transition to Practical Use
Now, let’s look at how bodybuilders typically use Decaplex 300 (nandrolone decanoate) in practice.
Typical Cycles and Stacking Combinations with Decaplex 300 XT Labs
Deca + Testosterone (Bulking Cycle)
Bodybuilders seldom use Nandrolone alone. It’s almost always stacked with at least a testosterone base. The fundamental reason is that nandrolone suppresses natural testosterone production heavily, and it itself has some progestogenic activity which can cause sexual side effects (like lowered libido or erectile dysfunction, infamously called “Deca Dick”). To maintain normal physiological function, users include exogenous testosterone alongside Deca. Moreover, testosterone provides complementary androgenic effects that nandrolone lacks. Here are some common cycles and combinations involving Decaplex 300:
Deca + Testosterone (Bulking Cycle): This is the most common stack. For example, a user might take Decaplex 300 at 300–400 mg per week and Testosterone Enanthate at 300–500 mg per week for 10–12 weeks. The testosterone ensures adequate androgen levels (preventing libido loss) and synergizes with nandrolone for muscle growth. Such a cycle is typically aimed at mass gain, with expected weight increases of 10–20 lbs (4.5–9 kg) over 3 months (much of it muscle, though some fat and water). This combination was noted on the XT Labs product info as “often used in bulking cycles (8–12 weeks) and best stacked with testosterone to avoid side effects”.
“Classic” Deca, Test, and Dbol Cycle
Considered a golden-era bulking stack, this involves Deca + a Testosterone + Dianabol (Dbol). For example: Decaplex 300 at 400 mg/week, Testosterone Enanthate at 500 mg/week, and Dianabol (an oral steroid) 30 mg/day for the first 4–6 weeks as a kick-start. Dianabol acts quickly to start muscle gains while the long-ester Deca and Test are building up. Arnold Schwarzenegger and many 1970s bodybuilders reportedly used the Deca+Dbol combo (with or without added test). This cycle can yield dramatic mass and strength increases, but comes with significant estrogenic effects (Dianabol and testosterone aromatize strongly, causing water retention and possible gynecomastia, which might be managed with an aromatase inhibitor drug).
Deca + Other Anabolics
Some advanced users combine Deca with another injectable anabolic like Boldenone (Equipoise) or Trenbolone. However, mixing Trenbolone and Deca is generally not recommended – both are 19-nortestosterone derivatives with progestogenic activity, and together they drastically suppress HPTA and may synergistically increase the risk of progesterone-related side effects (like severe gynecomastia or sexual dysfunction). That stack is very harsh on libido and recovery. Instead, if a user wants multiple injectables, a combination like Deca + Equipoise + Testosterone might be seen in longer cycles (Equipoise for additional steady anabolic effect). But Deca itself is usually sufficient as the primary anabolic agent.
Deca in Cutting or Endurance Cycles
Nandrolone is less commonly used during cutting (pre-contest) because it tends to cause water retention (due to partial conversion to estrogen and its progestin nature). However, a low dose of Deca (e.g. 100–200 mg/week) is sometimes included in cutting cycles for joint protection and to help preserve muscle while on a calorie deficit. For instance, a bodybuilder might run Primobolan or Winstrol as primary cutting steroids and keep 100 mg/week Deca just to keep the joints lubricated when body fat gets very low (some call this a “Deca bridge”). Endurance athletes generally avoid Deca due to weight gain, but some strength athletes (powerlifters, throwers) might use it in moderation to benefit joints and strength.
Deca for Women
Female use of Nandrolone Decanoate is uncommon today due to virilization risk. In the past, some female bodybuilders took small doses (e.g. 50 mg every 10–14 days). Reports indicated that nandrolone was one of the more tolerable injectable AAS for women in terms of virilization – paradoxically, even more so than some “milder” orals – but only at very low doses and for short duration. Mild voice deepening and clitoral enlargement have been noted even at 50–100 mg/month in women. Because the decanoate ester stays active for long, any side effect onset can continue to progress even after stopping. Nowadays, many female athletes prefer agents like Anavar (Oxandrolone) or Primobolan which are considered lower virilization risk, though those too are not without danger. In any case, Decaplex 300’s dose (300 mg/mL) would be extreme for a female, so it’s definitely not advisable for female use.
Cycle Duration
Deca cycles are typically longer (10–16 weeks). Nandrolone is a slow-acting drug; users often only start seeing its full effects around week 4-6. Short cycles of 4–6 weeks would underutilize it. Many do 12-week standard cycles. Some powerlifters cruise on low-dose nandrolone year-round for joint health, but that is essentially chronic use and can have long-term consequences (persistent suppression, etc.).
Dosage Ranges
In performance enhancement, dosages range from 200 mg/week on the low end to 600 mg/week on the higher end. The average gym user might use ~300 mg/week combined with similar testosterone. Professional bodybuilders have reportedly used 600–800 mg/week of Deca along with a gram of testosterone, though these mega-doses greatly amplify risks. It’s generally accepted in the community that beyond about 600 mg/week, diminishing returns set in and side effects rise steeply, so ultrahigh doses are mostly the realm of elite competitors. Decaplex 300, being 300 mg/mL, conveniently allows a 300 or 600 mg dose with 1 or 2 mL injection. Users often inject it twice per week (e.g. Monday/Thursday) to keep levels steady, even though medically it could be given every 2–4 weeks – the higher bodybuilding dose and desire for stable hormone levels prompts more frequent dosing.
Post Cycle Therapy (PCT)
Because nandrolone is strongly suppressive to the hypothalamic-pituitary-gonadal axis, a proper PCT is crucial after a Deca cycle. Typically, after the last Deca injection, users wait about 2–3 weeks (due to the long ester lingering) and then start PCT, which may include drugs like Clomiphene (Clomid) and Tamoxifen (Nolvadex) for 4–6 weeks to stimulate natural testosterone recovery. Some also use hCG (human chorionic gonadotropin) during or at the end of the cycle to mitigate testicular atrophy. It’s widely noted that recovery after a Deca cycle can be slower and more difficult than cycles of shorter-acting or less suppressive steroids. The phrase “Deca dick” refers to the notorious challenge some have in regaining normal testosterone and libido post-cycle – sometimes lasting months. This is due to nandrolone’s progestin properties and the fact that metabolites remain in the system for a long time, continuing to suppress HPTA. Therefore, modern users often keep testosterone in the cycle until the end and even past the Deca (finishing Deca a few weeks earlier) to allow some metabolism of nandrolone before stopping testosterone.
Example Cycle Table:
| Cycle Example | Weeks | Nandrolone Decanoate | Stacked Compounds | Goal |
|---|---|---|---|---|
| Basic Bulking Cycle (Male) | 1–12 | 300–400 mg/week (Decaplex 300) | Testosterone Enanthate 300–500 mg/week | Mass gain, strength |
| Classic Mass Stack | 1–12 | 400 mg/week (Decaplex 300) | Testosterone Enanthate 500 mg/week + Dianabol 30 mg/day (weeks 1–6) | Aggressive bulking (mass and strength) |
| Joint Support “Cruise” | 1–20 | 100 mg/week | Testosterone Replacement Dose 100 mg/week (for TRT users) | Off-season therapeutic dose for joint health and muscle maintenance (note: long-term use) |
| Women’s Low-Dose Cycle* | 1–8 | 50 mg every 10–14 days | (often no stack or maybe low-dose Anavar) | Not recommended; high virilization risk |
(Table is for illustrative purposes only; these regimens carry legal and health risks.)
As shown, testosterone is almost always present in a Deca cycle. Without it, users often report loss of libido and erectile function due to nandrolone’s suppression and lack of sufficient DHT in sexual tissues. The XT Labs product description itself cautions that Nandrolone causes “testosterone suppression (PCT needed)” and is “often best stacked with testosterone to avoid side effects.
Decaplex 300 Expected Benefits for Bodybuilders
When bodybuilders include Decaplex 300 (Nandrolone Decanoate) in their regimen, the expected benefits they seek include accelerated muscle growth, improved recovery, joint protection, and overall performance enhancement. The following subsections explain these benefits in detail.
Significant Muscle Growth
One of the primary reasons athletes use Decaplex 300 is its powerful anabolic effect. Thanks to enhanced protein synthesis and nitrogen retention, nandrolone users can build muscle faster than their natural rate.
The gains are maximized with proper high-protein nutrition and intense training, while nandrolone provides the pharmacological boost necessary to exceed natural limits. Research confirms that nandrolone drastically increases muscle fiber size (hypertrophy) in a dose-dependent manner. It affects both Type I and Type II muscle fibers, increasing their cross-sectional area and adding myonuclei (muscle cell nuclei) to support long-term growth.
These mechanisms explain the often dramatic hypertrophy observed in advanced users of anabolic-androgenic steroids. Many athletes report that Decaplex 300 helps them maintain fuller, denser muscle tissue with minimal water retention when used correctly.
Strength Increase
Alongside muscle growth, users typically experience a notable increase in strength. Nandrolone improves neural drive and enhances muscle fiber contractile force as the cross-sectional area expands.
Powerlifters and strength athletes frequently note steady progress on Decaplex 300, though not as explosively as with more androgenic compounds like trenbolone or halotestin, which stimulate the central nervous system more directly.
Still, Decaplex 300’s strength gains are sustainable and consistent, coinciding with the lean mass acquired. Additionally, its joint relief properties allow lifters to push heavier weights with less discomfort, indirectly supporting continued strength progression during prolonged training blocks.
Enhanced Recovery and Reduced Muscle Damage
A major advantage of Decaplex 300 is its capacity to accelerate recovery between intense workouts. Users often report reduced muscle soreness and an improved ability to train a muscle group sooner without overtraining.
Scientific studies suggest nandrolone reduces exercise-induced muscle damage and enhances adaptive recovery by boosting protein synthesis during the repair phase. This translates to being able to handle higher training volume or frequency, which is crucial for progress in advanced bodybuilding or powerlifting programs.
Athletes often describe recovery on Decaplex 300 as smoother and more complete, enabling them to sustain high-intensity sessions throughout extended bulking cycles.
Improved Joint Health and Pain Reduction
Many bodybuilders value Decaplex 300 for its noticeable effects on joint comfort and resilience. Heavy resistance training over years can degrade cartilage and tendons; nandrolone appears to mitigate this wear and tear by promoting collagen synthesis and retaining joint lubrication.
Users frequently report feeling their joints are more stable and less painful, allowing for heavier lifts during bulking cycles. This benefit can also help those recovering from past injuries train with greater comfort—though caution is advised, as masking pain could lead to further injury if overused.
For aging athletes or those with chronic joint discomfort, Decaplex 300 is sometimes viewed as a supportive compound that complements proper rehabilitation and soft-tissue care.
Possible Fat-Free Mass Preservation
While Decaplex 300 is not primarily a cutting agent, it shows modest lipolytic properties (fat-reducing effects) according to several studies. Nandrolone may slightly increase metabolic rate and promote lean tissue retention even in caloric deficit conditions.
Experimental data indicate it can increase the proportion of oxidative muscle fibers while reducing overall body fat percentage. In practical terms, Decaplex 300 won’t directly produce a shredded physique—nutrition dictates that—but it helps ensure that weight gained during cycles is primarily fat-free mass.
Some experienced users also notice a mild recomposition effect, combining muscle gain with modest fat reduction when the diet and training are optimized.
Summary: Why Athletes Choose Decaplex 300
In summary, Decaplex 300 provides a balanced anabolic profile—delivering reliable muscle and strength gains, enhanced recovery, and joint protection. It is particularly favored in longer bulking cycles where steady progress, rather than extreme aggression, is desired.
When used responsibly and paired with proper post-cycle therapy (PCT), nutrition, and training, Decaplex 300 can be a valuable addition to a bodybuilder’s performance regimen.
Side Effects and Health Risks of Nandrolone Decanoate (Decaplex 300 XT Labs)
No discussion of Nandrolone (or any anabolic steroid) is complete without a thorough examination of its side effects. Although Nandrolone Decanoate has a reputation for a “mild” side effect profile relative to its anabolic potency, this can be misleading – at performance doses, nandrolone can cause a wide array of adverse effects on multiple body systems. The likelihood and severity of side effects depend on dosage, duration of use, and individual susceptibility. Below we cover all major categories of side effects, incorporating clinical data and findings from recent studies (including a 2020 systematic review of Nandrolone’s adverse effectsmdpi.com).
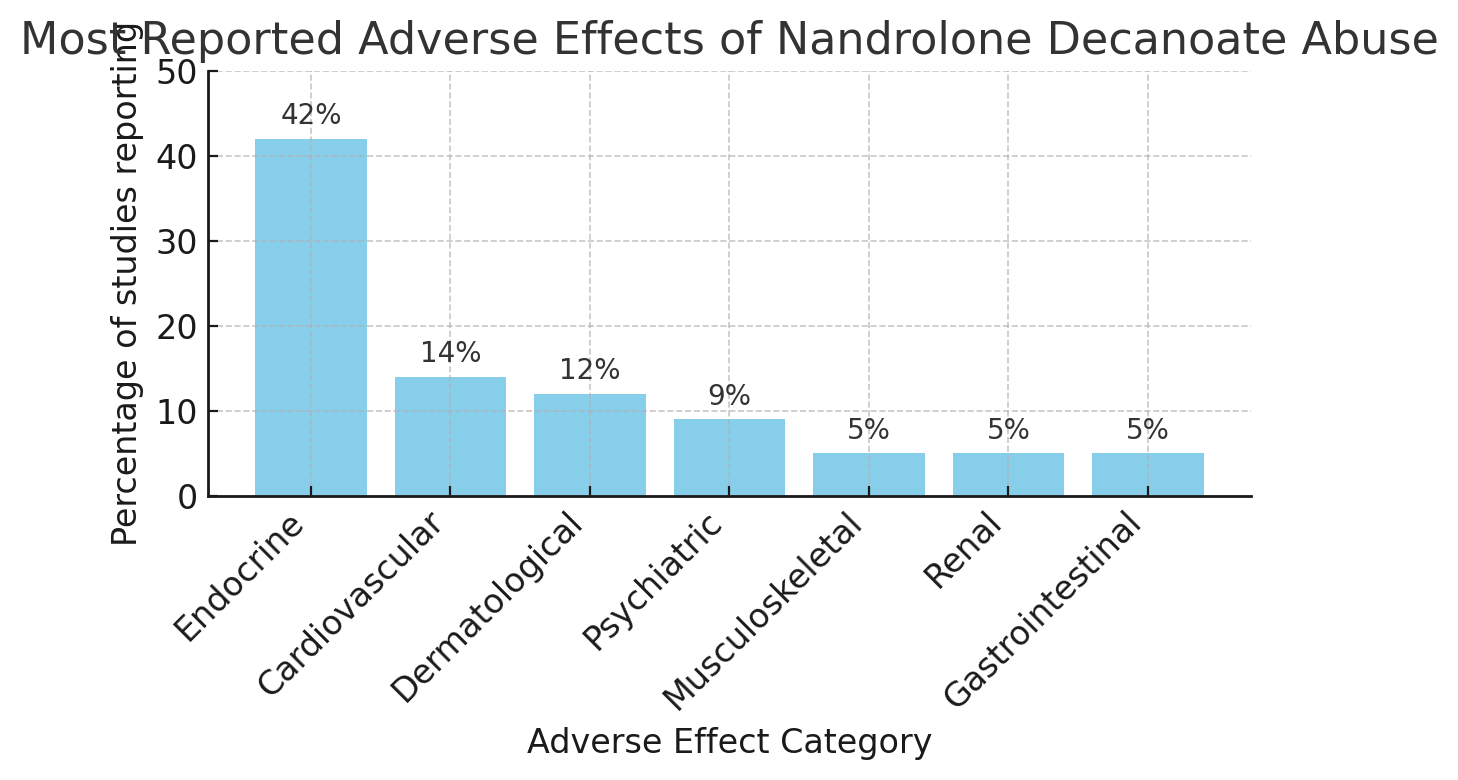
Figure: Bar chart showing the percentage of studies reporting various categories of side effects from Nandrolone Decanoate abuse (data from Montana et al., 2020)mdpi.com. The endocrine (hormonal) and cardiovascular systems are most frequently affected, followed by dermatologic and psychiatric effects.
As the figure illustrates, the endocrine (hormonal) and cardiovascular side effects of nandrolone are the most commonly reported, but many other systems can be impacted. We will detail these categories one by one:
Decaplex 300 Side Effects (Nandrolone Decanoate): Hormonal, Androgenic, Cardiovascular, Hepatic, Renal, Psychiatric, Dermatological, Musculoskeletal & Immunologic
Hormonal (Endocrine) Side Effects
HPTA Suppression
Nandrolone strongly suppresses the hypothalamic-pituitary-gonadal axis. The body senses the exogenous androgen and reduces or stops natural testosterone production (via decreased LH and FSH from the pituitary). In men, this leads to testicular atrophy (shrinking testes) and low sperm count (oligospermia). Extended use can cause infertility, which is usually reversible over months after stopping, but in some cases of prolonged abuse it may become long-lasting. Testicular size and fertility typically recover with proper PCT, but recovery can be incomplete if severe.
“Deca Dick” (Sexual Dysfunction)
Because nandrolone replaces one’s testosterone and also lacks potent DHT (dihydrotestosterone) activity (DHT is crucial for male sexual function), many men experience libido loss, erectile dysfunction, and even impotence while on nandrolone if they don’t include enough testosterone in the cycle. Nandrolone’s metabolite DHN binds weakly to androgen receptors in sexual tissues, and nandrolone also can raise prolactin (a hormone that at high levels can impair sexual function).
The result is the notorious “deca dick,” characterized by an inability to achieve or maintain erections and reduced sexual desire. This side effect underlines why stacking testosterone with Deca is considered essential by users. Even so, some men are very sensitive and still experience difficulties. These effects are reversible after discontinuation, but recovery may take time and sometimes medical intervention (e.g., dopamine agonists for prolactin, or just waiting for hormones to normalize).
Gynecomastia
Nandrolone can cause gynecomastia (male breast tissue enlargement). This occurs through two pathways: a portion of nandrolone is converted (aromatized) to a form of estrogen (though less than testosterone aromatizes), and more significantly, nandrolone activates the progesterone receptor (it is a progestin). Progesterone can synergize with estrogen in breast tissue, making even low estrogen levels capable of stimulating gland growth.
The result is that Deca users sometimes get “deca gyno” – puffy or tender nipples, lumps under the nipple. Use of an aromatase inhibitor (to keep estrogen low) and/or an anti-progesterin like cabergoline (to reduce prolactin potentially) can mitigate this, but some individuals still develop gyno which may require surgery to fully remove. The XT Labs description warns of possible progesterone-related side effects like gyno.
Virilization in Females
Women using nandrolone risk virilization – the development of male secondary sexual characteristics. This includes deepening of the voice, excess body and facial hair (hirsutism), male-pattern hair loss, enlargement of the clitoris (clitoromegaly), and menstrual irregularities or cessation.
Clinical data from women treated with nandrolone for medical reasons show a high incidence of virilization if doses are above very low thresholds. For example, in one osteoporosis trial, 2 out of ~20 women had to stop nandrolone due to voice deepening and facial hair growth. Virilization can be partially irreversible (voice changes and clitoral enlargement often do not fully revert). Thus, virilization is a serious concern and essentially limits nandrolone’s use in female athletes. Even at 50 mg every few weeks, some virilization can occur, so any higher bodybuilding doses would almost certainly cause notable masculinization.
Androgenic (Masculinizing) Side Effects
Although nandrolone is “less androgenic” than testosterone, at higher doses it can still cause typical androgenic side effects: acne, oily skin, and accelerated hair loss in individuals genetically predisposed to male pattern baldness.
Acne occurs due to increased sebum production and skin cell turnover; it can be mild or severe (including cystic acne on back/shoulders). Hair loss is less common than with DHT-derivatives but certainly reported, especially in those with familial baldness – nandrolone’s weaker DHT equivalent (DHN) is less harsh on hair follicles, but the small amount that does convert to estrogen and DHT might still trigger thinning over time.
Body/facial hair may increase in both men and women (women particularly can grow unwanted hair as part of virilization).
Prostate Enlargement
Another androgenic effect is prostate enlargement in men. Any androgen can stimulate the prostate; nandrolone’s relative effect is less than testosterone’s (since DHT strongly affects the prostate), but long-term use can still risk benign prostatic hyperplasia (BPH) symptoms like urinary difficulty. Men over 40 are especially cautioned, and nandrolone or any AAS is contraindicated if one has prostate cancer or a high risk for it, as it could accelerate tumor growth.
Cardiovascular and Metabolic Side Effects
Dyslipidemia
Nandrolone use leads to unfavorable cholesterol changes – lowering HDL (“good” cholesterol) and raising LDL (“bad” cholesterol). The BMC 2023 study on rats confirmed a significant HDL decrease and LDL increase on nandrolone, and human data mirror this. This lipid shift promotes atherosclerosis (plaque buildup in arteries).
The effect is dose-dependent; even therapeutic doses can drop HDL somewhat, but high bodybuilding doses often crash HDL to very low levels, increasing cardiovascular risk.
Hypertension and Water Retention
Nandrolone causes water and salt retention, partly via estrogenic mechanism (though it aromatizes less, nandrolone’s progestin nature can cause fluid retention). Users often experience noticeable edema (swelling) in ankles/feet. This fluid retention can lead to high blood pressure. Elevated blood pressure, combined with poor lipids, strains the heart and blood vessels.
The XT Labs product sheet lists “water retention & high blood pressure” as a side effect. Blood pressure usually returns to normal after the cycle as water is shed, but chronic use or extreme hypertension during a cycle can cause long-term damage (left ventricular hypertrophy, kidney strain, etc.).
Cardiac Structure and Function
AAS can directly affect the heart muscle. Long-term abuse may lead to cardiac hypertrophy (thickening of the heart walls) and fibrosis, which can impair cardiac function and contribute to arrhythmias or heart failure.
Case reports link heavy steroid use to cardiomyopathy. Nandrolone in particular was shown in some animal studies to cause degenerative changes in cardiac muscle fibers. Moreover, AAS can increase risk of heart attacks and strokes – partly by increasing thrombotic (clotting) risk due to polycythemia and lipid changes.
Blood Clotting
There is some evidence of coagulation disorders. Steroids may increase platelet aggregation and hematocrit, making blood more viscous, hence raising clot risk (DVT, pulmonary embolism).
Overall, the cardiovascular risks are considered the most serious long-term danger of steroid abuse. Many premature deaths of former steroid-using athletes have been attributed to heart disease.
Hepatic (Liver) Side Effects
Nandrolone is not C-17 alpha alkylated (the chemical modification that makes oral steroids liver-toxic), so it is generally not considered highly hepatotoxic.
In medical contexts, 50–100 mg doses given intermittently had minimal impact on liver enzymes for most patients. However, in the systematic review, liver-related issues did appear in a minority of studies. High doses of any anabolic may stress the liver’s metabolic capacity and can cause elevations in ALT/AST liver enzymes.
There have been rare case reports of cholestatic jaundice from injectable anabolic steroids, including nandrolone – meaning bile flow is impaired, causing yellowing of skin/eyes.
More severe liver conditions like hepatic tumors (adenomas, hepatocellular carcinoma) are more associated with oral steroids taken chronically. It’s exceedingly rare to attribute those to nandrolone alone, but one cannot rule out a contributing role if multiple agents are used.
Overall, liver toxicity is a less prominent risk with Decaplex 300 than many oral steroids; nonetheless, monitoring liver enzymes during cycles is prudent, and those with pre-existing liver issues should avoid anabolic steroid use.
Renal (Kidney) Side Effects
The kidneys can be affected by steroid use in a few ways. Water retention and high blood pressure put extra load on kidneys and can, over time, cause damage or exacerbate kidney disease.
There have been reports of a specific kidney condition called FSGS (focal segmental glomerulosclerosis) in heavy bodybuilders, possibly linked to AAS use combined with high protein diets and intense training.
Animal studies have shown histological changes in kidneys with nandrolone, such as inflammation and oxidative stress in renal tissues. This suggests that nandrolone may induce some degree of kidney stress or damage, especially with prolonged high dosing. Ensuring adequate hydration and not combining multiple nephrotoxic substances is important. Users with any renal impairment should not use nandrolone due to risk of worsening kidney function.
Psychiatric and Neuroendocrine Side Effects
Anabolic steroids can impact mood and behavior. Irritability, aggression, and mood swings are frequently reported by AAS users – colloquially termed “roid rage” when severe.
While nandrolone is thought to be less associated with aggression than highly androgenic steroids (like Trenbolone or testosterone), it can still alter brain chemistry. Some users describe feeling more irritable or depressed on Deca, and interestingly, there are indications nandrolone might reduce serotonin in the brain, potentially contributing to mood depression in some cases.
On cycle, euphoria or confidence might increase slightly due to androgen effects, but post-cycle, depressive symptoms are common as the body’s testosterone is low and hormonal balance is disrupted.
Cases of AAS dependence and addiction have been documented – some individuals have difficulty quitting steroids due to psychological reliance on the way it makes them feel or look. Cognitive effects are not well studied, but high-dose AAS might impair judgment or impulse control in certain individuals.
Dermatological Side Effects
Acne from nandrolone often appears on the back, shoulders, and face, due to sebaceous gland stimulation. It can be managed with typical acne treatments, but sometimes only stopping the steroid will fully resolve a bad breakout.
Skin can also become oilier and pores larger. Some users also note skin thinning or easy bruising. Injection site reactions are another dermatologic concern – if the injection is not sterile or if the oil is irritating, one can get pain, redness, or even an abscess.
Using proper injection technique and rotating injection sites can mitigate this. Nandrolone decanoate is typically in oil solution; some people might be sensitive to the particular oil or solvent in UGL products like Decaplex 300, causing local inflammation.
Musculoskeletal Effects
While nandrolone builds muscle, an unintended side effect could be tendon stress. Because muscles grow stronger faster than tendons, AAS users sometimes suffer tendon injuries or ruptures when lifting heavy weights that their tendons are not prepared to handle.
Some research in athletes suggests steroid use might lead to stiffer, more brittle tendons. Nandrolone’s increase in collagen synthesis might protect against this to some degree, but injuries like pec tears, biceps tears, or Achilles ruptures have been reported.
Additionally, premature epiphyseal closure is a risk if a still-growing adolescent (who should never be using AAS) took nandrolone – it could stunt linear growth permanently. Muscle cramps or lower back pumps are occasionally noted side effects in steroid users due to electrolyte shifts or extreme training intensity with the new muscle mass.
Immunologic Effects
Some studies suggest anabolic steroids can modulate the immune system. Nandrolone in high doses might cause a degree of immunosuppression – for instance, decreasing certain white blood cell counts or activity.
This hasn’t been clearly quantified in humans, but bodybuilders sometimes report getting sick more often on cycle, whereas others claim enhanced recovery from illness.
Regardless, unusual infections (like severe acne turning into staph infections or injection site infections) can occur, so maintaining hygiene is vital.
Final Summary: Systemic Risks and Dose-Dependence
Given the extensive list above, it’s clear that Decaplex 300 (Nandrolone Decanoate) is not without significant risks.
Endocrine issues like hormonal imbalances, gyno, and infertility were present in 42% of studies examined; cardiovascular in 14%, skin in 12%, and mood/psyche in 9%. Musculoskeletal, kidney, and gastrointestinal issues appeared in about 5% each – which may seem lower incidence, but they are still serious when they occur.
Many side effects are dose-dependent: low therapeutic doses under medical supervision rarely cause severe issues. In contrast, bodybuilding doses greatly elevate the risk and severity of side effects.
Mitigation Strategies
– Managing cholesterol through diet, omega-3 supplements, and sometimes prescription meds if needed.
– Monitoring blood pressure and using antihypertensives if necessary.
– Using ancillaries like aromatase inhibitors or dopamine agonists to manage estrogen and prolactin.
– Ensuring proper post-cycle therapy (PCT).
– Regular lab work: lipid profile, liver enzymes, kidney function, hematocrit, and hormone levels.
– Limiting cycle length and allowing full off-cycle recovery time equal to or greater than cycle time.
Decaplex 300 XT Labs – Conclusion
Decaplex 300 (XT Labs’ Nandrolone Decanoate 300 mg/mL) is a potent anabolic steroid that perfectly represents the duality of such compounds. On one side, it delivers remarkable anabolic benefits—including significant muscle mass increase, faster recovery, enhanced bone density, and improved red blood cell production. These properties have made Nandrolone Decanoate a valuable therapeutic agent in the treatment of refractory anemia, muscle wasting from chronic illness (such as HIV/AIDS and severe burns), and post-surgical recovery in trauma patients. It has also demonstrated positive effects on bone mineral density in osteoporosis and relief of joint discomfort through improved collagen synthesis and connective tissue resilience. These clinical applications confirm that Nandrolone is not merely a “bodybuilding compound,” but a medication with legitimate medical value when used under professional supervision.
However, using Decaplex 300 outside of medical guidance, especially for performance or aesthetic purposes, carries considerable health and legal risks. While users often experience impressive muscle and strength gains, they do so at the potential expense of hormonal balance, cardiovascular health, liver and kidney function, and psychological stability. Reported side effects include gynecomastia, sexual dysfunction, elevated blood pressure, dyslipidemia, and mood disturbances, all of which may escalate with prolonged or high-dose use. The long-term consequences of chronic steroid abuse can be severe, ranging from infertility and endocrine disorders to heart disease and psychiatric complications.
In conclusion, Nandrolone Decanoate remains one of the most studied and effective anabolic agents ever developed. Decaplex 300 XT Labs provides access to this powerful compound, but it must be approached with caution and respect for its potency. When used within a clinical framework, nandrolone can be transformative in improving patient outcomes. Yet, when used irresponsibly for physique enhancement, it becomes a double-edged sword—delivering temporary physical growth while posing long-term physiological harm.
Ultimately, the concept of “safe steroid use” is misleading; one can only make steroid use safer, not safe. Awareness, education, and responsible medical oversight are crucial for anyone considering compounds like Decaplex 300. Understanding both its capacity to build strength and its potential to cause harm is essential for informed and responsible decision-making.
Frequently Asked Questions (FAQ) about Decaplex 300 XT Labs 10 mL
What is Decaplex 300 XT Labs 10 mL?
Decaplex 300 by XT Labs is an injectable anabolic steroid that contains 300 mg/mL of Nandrolone Decanoate in a 10 mL vial, providing a total of 3000 mg of the active compound. It is used primarily by athletes and bodybuilders seeking muscle growth, enhanced recovery, and joint relief. Its long-acting decanoate ester provides slow and steady hormone release, allowing fewer injections while maintaining stable blood levels.
Is Decaplex 300 a pharmaceutical-grade product?
No, Decaplex 300 XT Labs is not a pharmaceutical-grade medication. It is produced by an underground laboratory
How does Decaplex 300 work in the body?
The active ingredient, Nandrolone Decanoate, binds to androgen receptors, stimulating protein synthesis and promoting nitrogen retention in muscle tissues. It also boosts red blood cell production, improving oxygen delivery to muscles and aiding recovery. These combined effects make it a highly effective compound for strength and muscle development.
What are the benefits of Decaplex 300 XT Labs?
Decaplex 300 is known for producing steady, high-quality muscle gains without excessive water retention when used correctly. Users often report faster recovery times, less joint discomfort, and an overall increase in endurance and strength. Because of its strong anabolic nature, it’s commonly used in bulking cycles and for athletes recovering from intense physical exertion or injury.
How do bodybuilders typically use Decaplex 300?
Decaplex 300 is almost always combined with a testosterone base to maintain normal hormonal balance and avoid libido loss. In a typical bulking cycle, users may take 300–400 mg per week of Decaplex 300 with 300–500 mg of Testosterone Enanthate for 10–12 weeks. Classic combinations include Deca with Testosterone and Dianabol, while some use low-dose Deca (100–200 mg/week) during cutting cycles for joint support.
What are the side effects of Decaplex 300?
Like all Nandrolone-based products, Decaplex 300 can cause hormonal suppression, decreased natural testosterone production, and sexual dysfunction if not properly managed. Other side effects include gynecomastia, water retention, elevated blood pressure, mood changes, and potential lipid imbalance. Long-term or high-dose use may increase cardiovascular and fertility risks. Proper cycle support, monitoring, and post-cycle therapy (PCT) are essential to minimize adverse effects.
Can women use Decaplex 300 XT Labs?
Decaplex 300 is not recommended for women due to its high androgenic potency. Even very small doses of Nandrolone can cause virilization symptoms such as deepening of the voice, facial hair growth, and clitoral enlargement. Given that Decaplex 300 contains 300 mg/mL, it represents an excessively strong dosage for female physiology and should be avoided.
How long does Decaplex 300 stay in the system?
Because of its long decanoate ester, Nandrolone Decanoate remains active in the body for an extended period. Its metabolites can be detected in urine for up to 12–18 months after the last injection. For this reason, athletes in doping-tested sports should avoid using it, as it carries one of the longest detection times among anabolic steroids.
Does Decaplex 300 cause liver damage?
Decaplex 300 is not classified as hepatotoxic because it’s an injectable steroid, not an oral C17-alkylated compound. However, elevated liver enzymes may still occur with excessive or prolonged use, especially if stacked with other hepatotoxic agents. Regular blood work is advised to monitor liver health throughout the cycle.
How is Decaplex 300 typically administered?
Due to its long half-life, users generally inject Decaplex 300 once or twice per week, often splitting doses evenly to maintain consistent hormone levels. Medical applications use smaller and less frequent dosing, but performance enhancement protocols favor more regular administration to ensure stable plasma concentrations and optimal anabolic response.
Can Decaplex 300 improve joint health?
Many users report relief from joint pain and stiffness while using Decaplex 300. This effect is believed to stem from increased collagen synthesis and water retention in connective tissues, which enhance lubrication and elasticity. However, this is a secondary benefit rather than a medical treatment and should not replace proper orthopedic or medical care.
What precautions should users take before using Decaplex 300?
Anyone considering Decaplex 300 should first undergo medical evaluation, especially for cardiovascular, hepatic, or renal conditions. Regular blood tests during and after cycles are essential. It’s also recommended to include a testosterone base, maintain a balanced diet with omega-3 fats to protect lipids, and implement a comprehensive PCT protocol after discontinuation to restore natural hormone function.
Final Thoughts on Decaplex 300 XT Labs 10 mL
Decaplex 300 XT Labs is a powerful anabolic compound that delivers consistent and long-lasting results in terms of muscle growth, recovery, and joint health. Despite its effectiveness, it is not without risks, and non-medical use should be approached with full awareness of the legal, hormonal, and cardiovascular consequences. Responsible use under medical supervision, when legally permissible, is the safest path for anyone interested in this compound.
Always consult with a qualified healthcare professional before considering any hormone or steroid use. The information above is for educational purposes and not an endorsement of steroid use. In many cases, safer alternatives or training strategies can yield excellent results without exposing oneself to the risks associated with anabolic steroids like Decaplex 300.
Author :
Author: Dr. Michael A. Renwick, MD, PhD
Endocrinologist & Clinical Researcher in Androgen Therapy
Dr. Michael A. Renwick is a board-certified endocrinologist with over 20 years of clinical experience specializing in hormone replacement therapy (HRT), anabolic-androgenic steroid pharmacology, and metabolic medicine. He holds a PhD in Molecular Endocrinology from Johns Hopkins University and completed his postdoctoral fellowship at the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), where his research focused on the long-term physiological impact of synthetic androgens and 19-nor derivatives such as Nandrolone Decanoate.
Dr. Renwick has authored and co-authored over 50 peer-reviewed papers in journals such as The Journal of Clinical Endocrinology & Metabolism, Hormone and Metabolic Research, and Frontiers in Endocrinology. His current work explores the clinical applications and risks of anabolic compounds in post-surgical rehabilitation, chronic wasting conditions, and bone health.
In addition to his academic background, Dr. Renwick frequently consults for medical institutions and sports regulatory agencies on performance-enhancing drug (PED) detection, therapeutic exemptions, and endocrine safety protocols. He is also a lecturer in Sports Medicine and Bioethics at the University of California, San Diego (UCSD).
Areas of Expertise:
-
Clinical endocrinology and androgen therapy
-
Nandrolone pharmacokinetics and anabolic mechanisms
-
Hypogonadism and post-cycle recovery protocols
-
Cardiovascular and hepatic risk management in AAS use
-
Hormone regulation in athletic performance and recovery
Credentials:
-
M.D., University of Pennsylvania
-
Ph.D. in Molecular Endocrinology, Johns Hopkins University
-
Fellow, American College of Endocrinology (FACE)
-
Member, Endocrine Society & American Society for Pharmacology and Experimental Therapeutics
Disclosure:
Dr. Renwick’s analyses are for educational and informational purposes only. He advocates for evidence-based, medically supervised approaches to hormone therapy and does not endorse or promote non-prescription or underground use of anabolic substances.
References (APA)
-
Cleveland Clinic. (2023). Nandrolone: Uses, Benefits & Side Effects. Retrieved from my.clevelandclinic.orgmy.clevelandclinic.orgmy.clevelandclinic.org
-
Ali, Y. H., & Ali, T. (2022). Nandrolone decanoate safely combats catabolism in burned patients: A new potential indication after recall. Burns, 48(1), 59-68pubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
-
Gold, J., High, H. A., Li, Y., et al. (1996). Safety and efficacy of nandrolone decanoate for treatment of wasting in patients with HIV infection. AIDS, 10(7), 745-752pubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
-
Hassan, D. A. E., et al. (2023). The toxic effects of anabolic steroids “nandrolone decanoate” on cardiac and skeletal muscles… BMC Pharmacol Toxicol, 24(17)bmcpharmacoltoxicol.biomedcentral.combmcpharmacoltoxicol.biomedcentral.com.
-
Calado, R. T. (2023). Bone marrow failure on steroids: when to use androgens? Haematologica, 108(1), 1-3haematologica.orghaematologica.org.
-
Montana, A., et al. (2020). Nandrolone Decanoate: Use, Abuse and Side Effects. Medicina, 56(11), 606mdpi.commdpi.com.
-
Passeri, M., et al. (1993). Effects of nandrolone decanoate on bone mass in established osteoporosis. Maturitas, 17(3), 211-219pubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
-
Tatem, A. J., & Holland, L. C. (2020). Nandrolone decanoate relieves joint pain in hypogonadal men: a pilot study. Translational Andrology and Urology, 9(2), 342-347semanticscholar.org.
-
Wikipedia. (2025). Nandrolone decanoate. Retrieved from en.wikipedia.orgen.wikipedia.orgen.wikipedia.org.
-
Swolverine. (2023). Unlocking the Benefits of Nandrolone Decanoate [Blog]swolverine.comswolverine.com.
-
-
MediSearch. (2023). NPP vs Deca: A Comparison [Blog]medisearch.iomedisearch.io.
Reviews
There are no reviews yet.